Cataract surgery is a procedure in which an eye doctor removes the clouded natural lens from the eye and replaces it with an artificial intraocular lens (IOL). It remains the only definitive treatment once cataracts significantly impair vision, and it is one of the most frequently performed surgeries worldwide.
This guide covers the causes and risk factors behind cataract development, the types of cataracts that affect the lens, surgical techniques and how they compare, what to expect before, during, and after the procedure, potential complications, and the role of IOL selection in visual outcomes.
Cataracts may develop from aging-related protein aggregation in the lens, but diabetes, cumulative UV exposure, eye injuries, long-term corticosteroid use, and inherited genetic factors can also contribute to lens clouding at varying rates and ages.
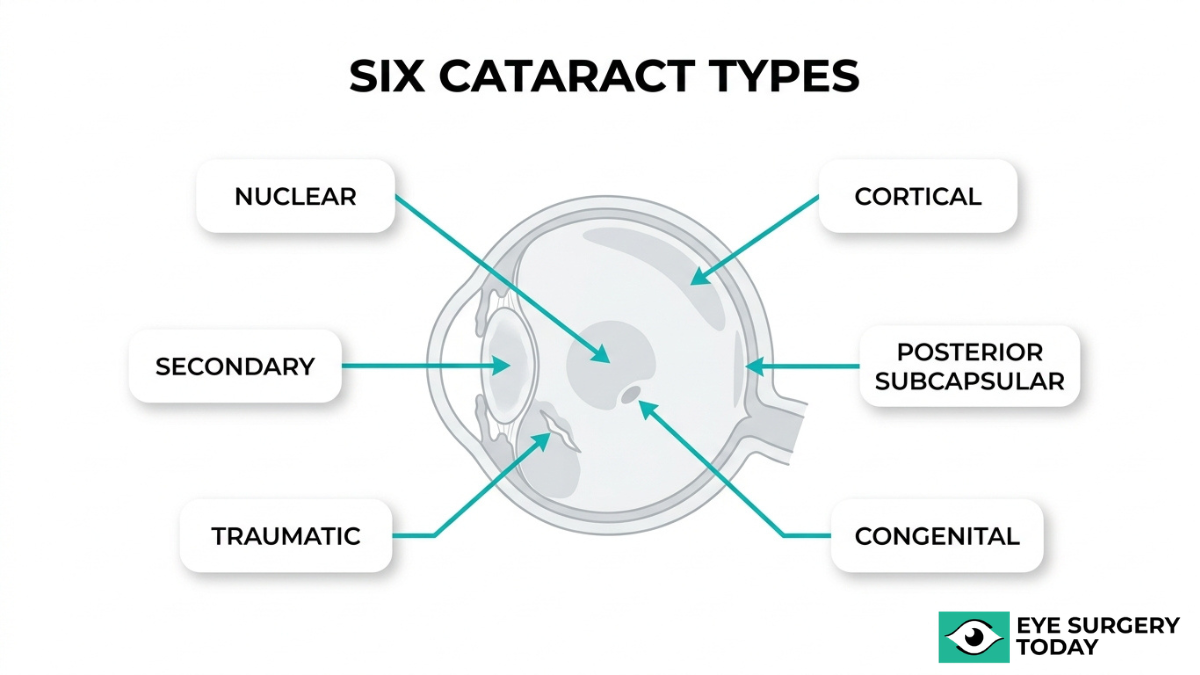
Six distinct cataract types, including nuclear sclerotic, cortical, posterior subcapsular, congenital, traumatic, and secondary, each form in different regions of the lens and progress at different speeds, which influences when surgical intervention may be appropriate.
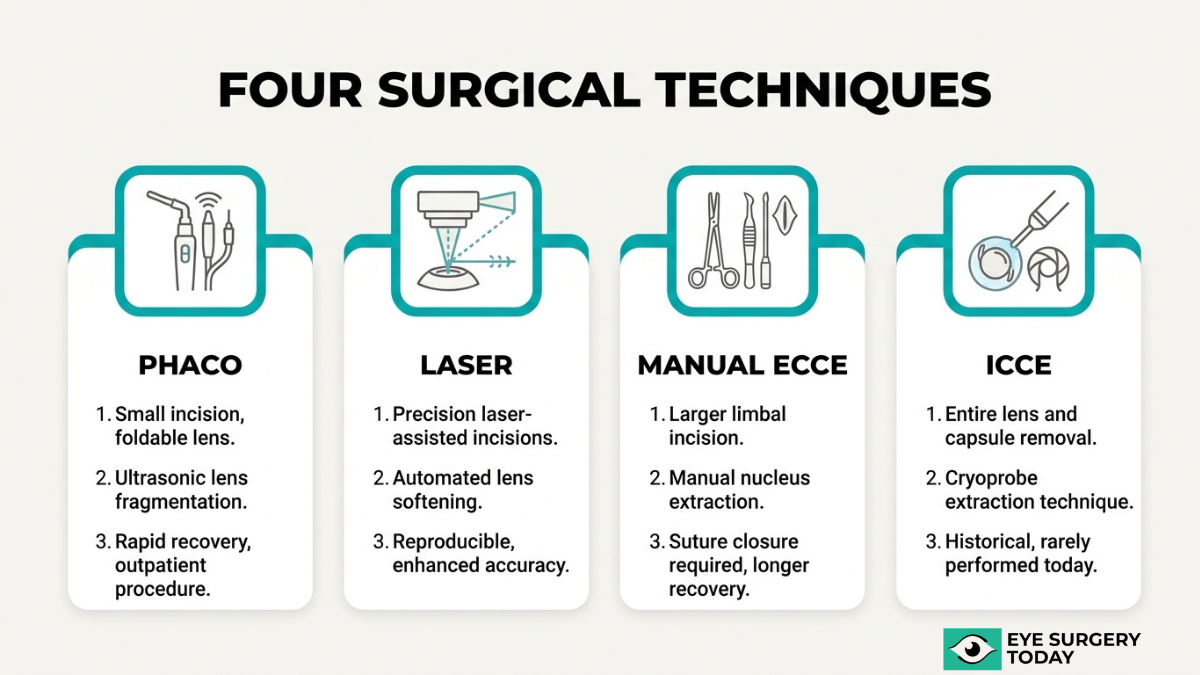
Phacoemulsification is the current standard of care, while femtosecond laser-assisted surgery, manual extracapsular extraction, and intracapsular extraction serve specific clinical scenarios. Cost-effectiveness, incision size, and cataract density all factor into technique selection.
The surgical experience itself is typically brief and performed under local anesthesia, with structured preoperative preparation and a recovery period spanning several weeks. Most patients may notice improved vision within days, though full stabilization can take longer.
Complications such as posterior capsule opacification, infection, retinal detachment, and elevated eye pressure vary in likelihood but are generally manageable with timely follow-up care. Selecting the right IOL, whether monofocal, multifocal, or extended depth-of-focus, directly shapes post-surgical visual quality and spectacle dependence.
What Is Cataract Surgery?
Cataract surgery is a procedure in which an eye doctor removes the clouded natural lens from the eye and replaces it with an artificial lens called an intraocular lens, or IOL. According to the National Eye Institute, during surgery, your eye doctor will remove the cloudy lens from your eye and replace it with an artificial lens. This outpatient procedure is one of the most frequently performed surgeries worldwide, driven by the scale of cataract-related vision loss. In 2020, cataracts accounted for 17.0 million cases of blindness and 83.5 million cases of moderate-to-severe vision impairment globally, as reported by the Institute for Health Metrics and Evaluation. Because cataracts cannot be reversed with medication or corrective lenses once they significantly impair vision, surgical removal of the affected lens remains the only definitive treatment. The procedure typically takes less than 30 minutes per eye, and most patients return home the same day. Understanding what cataract surgery involves is the first step toward making a confident, informed decision about vision correction.
What Causes Cataracts to Develop?
Cataracts develop from a combination of aging, medical conditions, environmental exposure, injury, medications, and inherited genetic factors. The following sections explain each cause in detail.
How Does Aging Contribute to Cataract Formation?
Aging contributes to cataract formation through gradual protein breakdown inside the eye lens. Over time, the crystallin proteins that keep the lens clear begin to clump together, creating cloudy areas that scatter light and reduce vision. According to a study published in Investigative Ophthalmology & Visual Science, cataract is caused by protein-protein and protein-membrane aggregation in the eye lens, with extensive binding of crystallins to lens cell membranes occurring after middle age.
This process is slow and progressive. Most people do not notice early lens changes, which is why routine eye exams become increasingly important with age. By the time symptoms like blurred vision or glare sensitivity appear, the cataract may have been forming for years.
How Does Diabetes Contribute to Cataract Formation?
Diabetes contributes to cataract formation by altering the chemical environment inside the eye lens. Elevated blood sugar levels can cause sorbitol to accumulate within lens fibers, leading to osmotic swelling and structural damage that accelerates lens clouding.
The risk is substantial. According to a 2023 review in the Journal of Clinical Medicine, cataracts occur two to five times more frequently in patients with diabetes, and this frequency can increase by 15 to 25 times in individuals under 40 years of age. For diabetic patients, early and consistent monitoring of lens health is one of the most practical steps toward preserving long-term vision.
How Does UV Exposure Contribute to Cataract Formation?
UV exposure contributes to cataract formation by generating oxidative stress in the lens, which damages proteins and accelerates clouding over time. Cumulative ultraviolet radiation, particularly UV-B, is a well-established environmental risk factor.
The dose-response relationship is striking. A study published in PLOS ONE found that sun exposure had a significant association with cataract, with odds ratios increasing from 1.6 in the third quintile of exposure to 9.4 in the fifth quintile (p<0.0001). Wearing UV-blocking sunglasses and wide-brimmed hats represents one of the simplest, most effective preventive measures available.
How Do Eye Injuries Contribute to Cataract Formation?
Eye injuries contribute to cataract formation by physically disrupting the lens capsule or lens fibers, allowing aqueous humor to penetrate and cause swelling and opacification. Blunt force trauma, penetrating wounds, and chemical burns can all trigger this process.
Traumatic cataracts may develop immediately after an injury or years later. According to StatPearls (NCBI), up to 65% of eye traumas lead to cataract formation, resulting in significant short- and long-term vision loss. Even seemingly minor eye injuries warrant follow-up evaluation, since delayed cataract development is common and often overlooked.
How Do Medications Like Corticosteroids Contribute to Cataracts?
Medications like corticosteroids contribute to cataracts by altering lens metabolism and promoting protein aggregation, particularly in the posterior subcapsular region of the lens. Both systemic and inhaled corticosteroids carry this risk when used over extended periods.
According to a 2023 pooled analysis published in the Journal of Ophthalmology (Hindawi), corticosteroid-exposed asthma and COPD patients faced on average a doubled risk of cataract, with daily high-dose inhaled corticosteroid use at or above 1000 micrograms associated with a significant risk of developing cataracts. Patients on long-term corticosteroid therapy should discuss regular lens monitoring with their eye care provider.
How Do Genetics Contribute to Cataract Formation?
Genetics contribute to cataract formation through inherited mutations affecting lens proteins, membrane channels, and developmental pathways. Congenital cataracts, present at birth or developing in early childhood, often result from autosomal dominant gene mutations.
According to a 2025 study in BMC Medical Genomics, the global prevalence of congenital cataract is estimated to range from 0.63 to 9.74 per 10,000 individuals. Beyond congenital forms, family history of age-related cataracts may also increase an individual’s susceptibility. While genetic predisposition cannot be modified, awareness of family history helps guide earlier screening and more proactive monitoring.
Understanding these causes helps inform the conversation about cataract types, which the next section explores.
What Are the Types of Cataracts?
The types of cataracts are nuclear sclerotic, cortical, posterior subcapsular, congenital, traumatic, and secondary. Each type differs in where it forms within the lens and what causes it.
Nuclear Sclerotic Cataract
A nuclear sclerotic cataract is a clouding that develops in the central zone, or nucleus, of the eye’s natural lens. This type progresses gradually over years, often causing the lens to harden and turn yellow or brown. Early on, some individuals notice a temporary improvement in near vision, sometimes called “second sight,” before distance vision worsens. Nuclear sclerotic cataracts are the most commonly diagnosed age-related cataract type. Because they develop slowly, many people adapt to the subtle vision changes without realizing a cataract is forming until it begins interfering with daily activities like driving at night.
Cortical Cataract
A cortical cataract forms in the outer edge, or cortex, of the lens and extends inward with white, wedge-shaped opacities. These spoke-like streaks scatter incoming light, often causing glare and difficulty with contrast. According to a study published in JAMA Ophthalmology, the three-year cumulative incidence for persons aged 65 to 74 was 18% for cortical cataracts, making this the most frequently occurring subtype in that age group. Individuals with diabetes may face a higher risk of developing cortical lens changes. Because glare is a hallmark symptom, people with cortical cataracts often struggle most in bright sunlight or when facing oncoming headlights.
Posterior Subcapsular Cataract
A posterior subcapsular cataract forms on the back surface of the lens capsule, directly in the path of light entering the eye. This positioning causes disproportionate vision interference relative to the cataract’s size, particularly affecting reading vision and creating halos around lights at night. Posterior subcapsular cataracts tend to progress faster than nuclear or cortical types, sometimes developing over months rather than years. Long-term corticosteroid use and diabetes are notable risk factors. For patients who rely heavily on near vision or who drive frequently at night, this subtype often warrants earlier surgical evaluation than slower-forming cataracts.
Congenital Cataract
A congenital cataract is a lens opacity present at birth or developing during early childhood. According to a 2025 review in BMC Medical Genomics, the global prevalence of congenital cataracts is estimated to range from 0.63 to 9.74 per 10,000 individuals, with a median of 1.71. Genetic mutations, intrauterine infections such as rubella, and metabolic disorders can all contribute to their formation. Early detection is critical because an untreated congenital cataract may lead to amblyopia, a condition where the visual pathways fail to develop properly. Pediatric ophthalmologists typically recommend prompt intervention when the opacity significantly obstructs the visual axis.
Traumatic Cataract
A traumatic cataract develops after a blunt or penetrating injury to the eye damages the lens structure. The onset can be immediate following the trauma or may appear months to years later as disrupted lens fibers gradually lose transparency. Traumatic cataracts can occur at any age, distinguishing them from most age-related forms. Surgical planning for this subtype often requires additional considerations, such as managing concurrent damage to the iris, capsule, or zonular fibers that support the lens. This complexity makes preoperative imaging and careful surgical technique especially important.
Secondary Cataract
A secondary cataract refers to lens opacification that develops as a consequence of another medical condition, medication, or prior eye surgery. Diabetes, prolonged corticosteroid use, and previous intraocular procedures are among the most common contributing factors. The term is also sometimes used informally to describe posterior capsule opacification, which can occur after cataract surgery when residual cells cloud the capsule holding the intraocular lens. Unlike true cataract recurrence, posterior capsule opacification is typically treated with a quick, noninvasive YAG laser capsulotomy rather than a second surgery.
With cataract types clarified, the next section covers the main surgical techniques used to treat them.
What Are the Main Cataract Surgery Techniques?
The main cataract surgery techniques are phacoemulsification, femtosecond laser-assisted cataract surgery, manual extracapsular cataract extraction, and intracapsular cataract extraction.
Phacoemulsification
Phacoemulsification is the most widely performed cataract surgery technique worldwide. The procedure uses ultrasonic energy to break the clouded natural lens into small fragments, which are then suctioned from the eye through a tiny incision. Because the incision typically measures around 2 to 3 millimeters, it often requires no stitches and promotes faster healing. After lens removal, the surgeon implants an intraocular lens (IOL) through the same micro-incision. This small-incision approach generally results in less surgically induced astigmatism compared to larger-incision methods. For most patients with routine cataracts, phacoemulsification remains the standard of care due to its proven safety profile and predictable visual outcomes.
Femtosecond Laser-Assisted Cataract Surgery
Femtosecond laser-assisted cataract surgery (FLACS) uses a precision femtosecond laser to perform key steps of the procedure, including corneal incisions, capsulotomy, and initial lens fragmentation. The laser’s image-guided technology can create highly reproducible incision patterns, which may benefit complex cases requiring precise capsulotomy placement. However, large randomized controlled trials conducted in the United Kingdom and France reported that FLACS was less cost-effective than phacoemulsification, according to a review cited by the American Society of Cataract and Refractive Surgery. While the technology adds precision to certain surgical steps, overall safety and efficacy outcomes remain comparable to standard phacoemulsification for most patients. FLACS may be a reasonable option when specific anatomical factors warrant enhanced surgical control, though the added cost is an important consideration.
Manual Extracapsular Cataract Extraction
Manual extracapsular cataract extraction (ECCE) is a technique that removes the clouded lens in one piece through a larger incision, typically 9 to 13 millimeters. Surgeons preserve the posterior lens capsule to support IOL placement. According to the American Academy of Ophthalmology, phacoemulsification is far more dependent on technology than conventional ECCE and more costly. This makes ECCE particularly valuable in resource-limited settings where advanced phacoemulsification equipment may be unavailable. The technique also remains useful for very dense or mature cataracts that resist ultrasonic fragmentation. Although the larger incision requires sutures and recovery may take longer, ECCE continues to serve an important role in global cataract care.
Intracapsular Cataract Extraction
Intracapsular cataract extraction (ICCE) removes the entire lens along with its surrounding capsule through a large incision. Because no capsular support remains, the IOL must be placed in the anterior chamber or fixated to the iris or sclera. This technique is rarely performed today, having been largely replaced by methods that preserve the posterior capsule. ICCE may still be considered in rare situations involving significant lens subluxation or zonular weakness where capsular support is absent. The larger wound size increases the risk of complications, including astigmatism and vitreous loss. Modern cataract surgery has moved decisively toward smaller-incision techniques, making ICCE a historical approach reserved for exceptional circumstances.
With surgical techniques established, understanding how phacoemulsification compares directly to laser-assisted surgery can help clarify which approach may suit different clinical needs.
How Does Phacoemulsification Compare to Laser-Assisted Surgery?
Phacoemulsification compares to laser-assisted surgery through differences in technique, precision, cost, and clinical outcomes. Both methods effectively treat cataracts, though each carries distinct advantages.
Phacoemulsification uses ultrasonic energy to break apart the cloudy lens through a small incision created manually by the surgeon. This technique has been the standard of care for decades, offering well-established safety data and broad availability. Surgeons control each step directly, from capsulorhexis to lens fragmentation and aspiration.
Femtosecond laser-assisted cataract surgery (FLACS) automates several key steps. The laser creates precise corneal incisions, performs the capsulotomy, and softens the lens before aspiration. This automation may improve capsulotomy circularity and reduce the ultrasound energy needed during lens removal, which can benefit patients with dense cataracts or complex anatomy.
Despite these technical refinements, clinical outcomes between the two procedures remain comparable for most patients. According to a report from Review of Optometry, large randomized controlled trials in the United Kingdom and France found that FLACS was less cost-effective than phacoemulsification.
Key differences include:
- Incision creation: Manual blade in phacoemulsification; femtosecond laser in FLACS.
- Capsulotomy precision: Surgeon-dependent in phacoemulsification; laser-guided in FLACS, which may offer more consistent circularity.
- Ultrasound energy: Typically higher in standard phacoemulsification; reduced in FLACS due to laser pre-fragmentation.
- Cost: Phacoemulsification is generally less expensive; FLACS involves additional equipment fees.
- Surgical time: Phacoemulsification can be faster overall; FLACS adds a separate laser step before phacoemulsification is completed.
For most routine cataracts, phacoemulsification delivers excellent results at a lower cost. FLACS may offer marginal benefits in specific clinical scenarios, but the added expense often outweighs those advantages for straightforward cases. The choice between these techniques ultimately depends on individual eye anatomy, cataract complexity, and surgeon recommendation. Regardless of the chosen technique, modern advancements in anesthesia and surgical precision ensure that cataract surgery is pain-free and safe for the vast majority of patients.
Understanding how these techniques compare can help when evaluating candidacy requirements with your eye care provider.
Who Is a Good Candidate for Cataract Surgery?
A good candidate for cataract surgery is someone whose cataracts significantly impair daily vision and quality of life. Candidacy depends on symptom severity, overall eye health, and individual medical factors.
Most people with cataracts do not need surgery immediately. Your ophthalmologist may recommend the procedure when lens clouding interferes with essential activities, such as driving, reading, or working. Updated prescriptions and stronger lighting can manage early symptoms, but surgery becomes the primary option once these measures no longer help.
Several factors may determine whether someone is a suitable candidate:
- Vision impacts daily function. Difficulty with routine tasks like driving at night, recognizing faces, or reading despite corrective lenses often signals that surgery should be considered.
- Conservative measures are no longer effective. When new glasses, magnification, or improved lighting fail to restore adequate vision, surgical lens replacement may be the next step.
- Overall eye health supports the procedure. Conditions such as uncontrolled glaucoma, active eye infections, or severe macular degeneration may need to be managed before cataract surgery can proceed safely.
- Systemic health conditions are stable. Patients with diabetes or those taking blood-thinning medications can often undergo cataract surgery, provided these conditions are well controlled under a physician’s guidance.
- The patient has realistic expectations. Understanding that intraocular lens selection affects visual outcomes, and that some patients may still need glasses after surgery, is an important part of candidacy.
According to the Mayo Clinic, about 9 out of 10 people who get cataract surgery see better afterward, though vision may be blurry at first while the eye recovers. This high success rate makes the procedure one of the most reliable elective surgeries available, but it works best when the timing aligns with a patient’s functional needs rather than cataract size alone.
Ultimately, candidacy is not determined by age or cataract type alone. A thorough preoperative evaluation, including measurements for IOL selection and a review of medical history, helps your eye doctor determine whether the benefits outweigh the risks for your specific situation. Knowing what to expect before surgery can help you prepare for each step of the process.
What Should You Expect Before Cataract Surgery?
Before cataract surgery, you should expect a comprehensive preoperative evaluation, specific medication instructions, and lifestyle adjustments in the days leading up to your procedure. These preparations help your surgeon plan the safest, most effective approach for your eye.
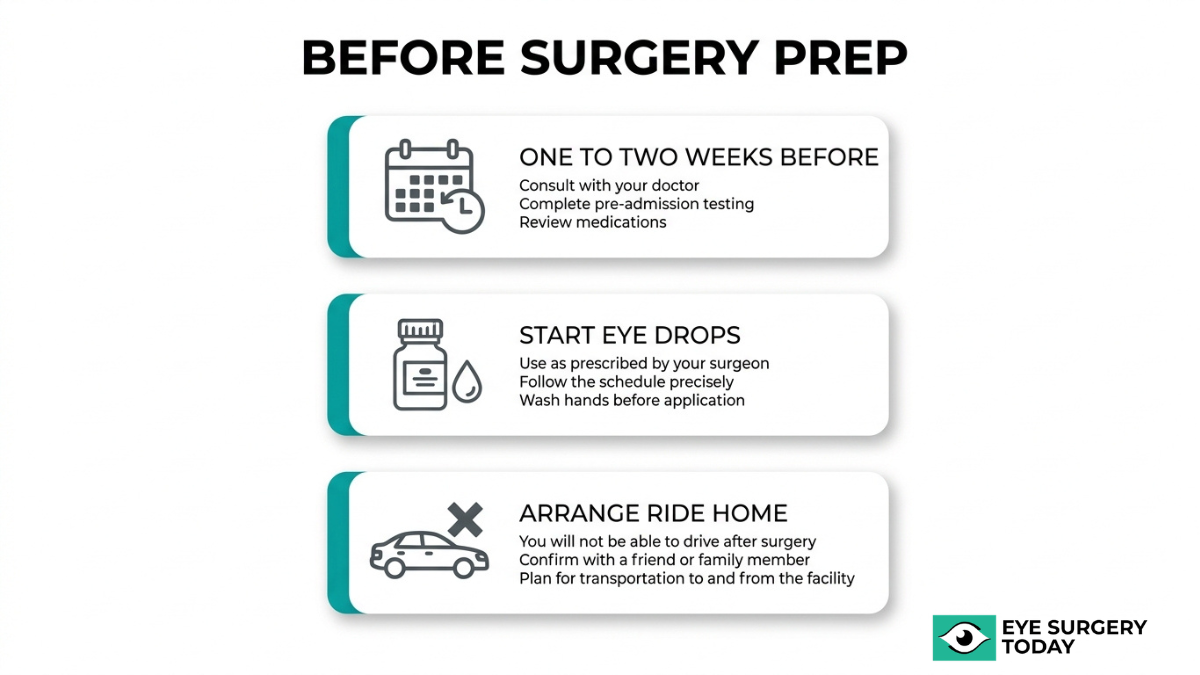
Your ophthalmologist will typically schedule a detailed eye examination one to two weeks before surgery. During this visit, several key measurements and assessments take place:
- Biometry testing measures the length of your eye and the curvature of your cornea, which determines the correct intraocular lens (IOL) power.
- Pupil dilation allows your surgeon to examine the lens and retina thoroughly.
- Eye pressure measurement establishes a baseline reading for comparison after surgery.
- Review of current medications, since blood thinners and certain supplements may need to be paused.
Your surgeon may prescribe antibiotic or anti-inflammatory eye drops to begin using one to three days before the procedure. These drops help reduce infection risk and prepare the eye’s surface. You will also receive instructions to avoid eating or drinking for several hours before surgery, as most procedures involve light sedation.
Because cataract surgery typically addresses one eye at a time, arranging transportation home is essential. The sedation and temporary visual changes make driving unsafe on the day of the procedure. This preparation phase, while straightforward, plays a direct role in surgical outcomes and recovery comfort. With preoperative steps completed, understanding what happens during the procedure itself becomes the next focus.
What Should You Expect During Cataract Surgery?
During cataract surgery, you should expect a short outpatient procedure where your surgeon removes the clouded natural lens and replaces it with an artificial intraocular lens (IOL). The entire process typically takes 15 to 30 minutes per eye, and most patients remain awake under local anesthesia.
Before the procedure begins, the surgical team applies numbing eye drops to eliminate pain. A mild sedative may also be offered to help you relax. Once the anesthetic takes effect, a small instrument called a lid speculum holds the eye open, so blinking is not a concern during the operation.
Your surgeon then creates a tiny incision in the cornea. Through this opening, the clouded lens is broken apart using ultrasound energy (phacoemulsification) or a femtosecond laser, depending on the chosen technique. The fragmented lens material is gently suctioned out. According to the National Eye Institute, your eye doctor will remove the cloudy lens and replace it with an artificial lens, called an intraocular lens or IOL. This replacement lens is folded, inserted through the same micro-incision, and positioned inside the natural lens capsule, where it unfolds permanently into place.
Most patients experience little to no discomfort during the procedure. You may notice bright lights or slight pressure, but pain is rare. Because the incision is self-sealing in most cases, stitches are usually unnecessary. After a brief observation period in the recovery area, you can typically go home the same day with a protective eye shield.
Understanding what happens during the procedure can help ease anxiety, and knowing what recovery involves is the next important step.
What Should You Expect During Recovery After Cataract Surgery?
Recovery after cataract surgery typically spans several weeks, with most patients noticing improved vision within a few days. Similar to other eye procedures, Similar to other eye procedures, the healing process involves managing mild discomfort, following prescribed eye drop regimens, and attending follow-up appointments. According to the Mayo Clinic, about 9 out of 10 people who get cataract surgery see better afterward, but vision may be blurry at first while the eye recovers.
During the first 24 to 48 hours, mild itching, light sensitivity, and watery eyes are common. These symptoms generally resolve on their own as healing progresses. Your ophthalmologist will likely prescribe antibiotic and anti-inflammatory eye drops to reduce the risk of infection and control swelling.
Key recovery guidelines typically include:
- Avoiding rubbing or pressing on the operated eye.
- Wearing the protective eye shield, especially while sleeping, for the first week.
- Refraining from heavy lifting and strenuous activity for at least two weeks.
- Keeping water and soap away from the eye during bathing.
- Attending all scheduled post-operative visits so the surgeon can monitor healing.
Most patients can return to light daily activities within a few days, though full stabilization of vision may take four to six weeks. Colors often appear brighter after surgery because the new intraocular lens is clear, unlike the cloudy natural lens that was removed.
It is worth noting that some visual fluctuations during the first few weeks are normal and do not necessarily indicate a problem. However, sudden symptoms such as severe pain, significant vision loss, or flashing lights should prompt immediate contact with the surgical team, as these could signal rare but serious complications. Patience during this period pays off; for most individuals, the final visual outcome represents a substantial improvement in daily quality of life.
Understanding what normal recovery looks like helps distinguish expected symptoms from signs that may need urgent attention.
What Are the Potential Risks and Complications of Cataract Surgery?
The potential risks and complications of cataract surgery include posterior capsule opacification, infection, retinal detachment, swelling, lens dislocation, and elevated eye pressure. Each complication varies in likelihood and severity.
What Is Posterior Capsule Opacification After Cataract Surgery?
Posterior capsule opacification (PCO) is a condition where the thin membrane left behind the intraocular lens becomes cloudy after cataract surgery, causing vision to blur again. According to the American Society of Cataract and Refractive Surgery, PCO is the most common long-term complication of cataract surgery, with reported incidence rates often cited between 20% and 50% within two to five years postoperatively.
Residual lens epithelial cells can proliferate and migrate across the posterior capsule, gradually scattering light before it reaches the retina. Symptoms often resemble the original cataract, including hazy or foggy vision and increased glare sensitivity.
PCO is treated with a quick, painless outpatient procedure called YAG laser capsulotomy, which creates a small opening in the clouded capsule to restore clear vision. While PCO is common, it remains one of the most straightforward complications to correct, and most patients notice improved clarity within a day or two of treatment.
What Is the Risk of Infection After Cataract Surgery?
The risk of infection after cataract surgery is very low but carries serious consequences if it occurs. Endophthalmitis, a severe intraocular infection, has an estimated incidence rate of approximately 0.04% to 0.12%, according to the British Journal of Ophthalmology.
Symptoms of postoperative endophthalmitis may include sudden pain, redness, swelling, and rapidly declining vision, typically within the first week after surgery. Prompt treatment with intravitreal antibiotics is critical to preserving sight. Surgeons reduce infection risk through preoperative antiseptic protocols, sterile technique, and prophylactic antibiotic drops prescribed before and after the procedure.
Although the probability is low, this complication underscores why patients should report any sudden changes in comfort or vision to their eye care provider immediately rather than waiting for a scheduled follow-up.
What Is the Risk of Retinal Detachment After Cataract Surgery?
The risk of retinal detachment after cataract surgery is small, though it may be slightly elevated compared to the general population. During cataract removal, changes in the vitreous gel can increase traction on the retina, potentially leading to a tear or detachment in susceptible individuals.
Patients who are highly myopic or have a history of retinal problems may face a higher likelihood. Warning signs include sudden flashes of light, a noticeable increase in floaters, or a shadow spreading across the visual field. Because retinal detachment can cause permanent vision loss if untreated, any of these symptoms warrants immediate evaluation. Early surgical intervention, such as vitrectomy or pneumatic retinopexy, can often reattach the retina and preserve functional vision.
What Is the Risk of Swelling or Edema After Cataract Surgery?
The risk of swelling or edema after cataract surgery primarily involves a condition called cystoid macular edema (CME). CME occurs when fluid accumulates in the macula, the central part of the retina responsible for sharp, detailed vision.
Mild corneal swelling is also common in the first few days after surgery and typically resolves on its own. CME, however, may develop weeks later, causing blurred or distorted central vision. Anti-inflammatory eye drops, including nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids, are the standard preventive and treatment approach. Most cases of postoperative CME respond well to medical therapy and resolve within several months, though persistent cases may require additional intervention.
What Is the Risk of Dislocated Intraocular Lens After Surgery?
The risk of a dislocated intraocular lens (IOL) after surgery is uncommon but can affect visual quality if it occurs. During cataract surgery, the cloudy natural lens is removed and replaced with an artificial intraocular lens, which is positioned inside the remaining capsular bag.
IOL dislocation may happen if the capsular bag or the zonular fibers supporting it weaken over time. Risk factors include trauma to the eye, pseudoexfoliation syndrome, and previous ocular surgery. Symptoms can range from subtle visual disturbances to significant vision changes depending on the degree of displacement. Surgical repositioning or IOL exchange can correct the problem when it significantly affects vision.
What Is the Risk of Elevated Eye Pressure After Surgery?
The risk of elevated eye pressure after surgery is a recognized short-term complication of cataract removal. Intraocular pressure (IOP) may spike in the first 24 to 48 hours following the procedure due to retained viscoelastic material, inflammation, or debris blocking the eye’s drainage pathways.
For most patients, the pressure increase is temporary and resolves with medicated eye drops. However, patients with pre-existing glaucoma face a higher risk of sustained IOP elevation and may require closer monitoring. Left untreated, persistently high eye pressure can damage the optic nerve over time. Routine postoperative pressure checks allow early detection, making this complication highly manageable when follow-up care is maintained.
Understanding these surgical risks helps patients prepare for informed conversations with their eye care provider about IOL selection and expected outcomes.
What Role Does IOL Selection Play in Cataract Surgery Outcomes?
IOL selection plays a central role in cataract surgery outcomes by determining the range and quality of vision after the procedure. The following sections cover how surgeon-reviewed guides can support your decision and the key takeaways about cataract surgery procedures.
How Can Surgeon-Reviewed IOL Guides Help You Choose?
Surgeon-reviewed IOL guides can help you choose by breaking down complex lens options into clear, comparable categories matched to your vision goals and lifestyle. Monofocal IOLs provide clear vision at one distance, while multifocal and extended depth-of-focus (EDOF) IOLs aim to reduce spectacle dependence by offering vision at multiple distances. Understanding these distinctions before your consultation allows for a more productive conversation with your eye doctor.
A reliable guide should cover lens material, optical design, and which refractive errors each IOL type corrects. Eye Surgery Today offers surgeon-reviewed educational resources, including IOL comparison guides, designed to help patients evaluate their options with confidence. For most patients, matching the right IOL to daily visual demands matters as much as the surgical technique itself.
What Are the Key Takeaways About Cataract Surgery Procedures?
The key takeaways about cataract surgery procedures are that modern techniques are safe, effective, and highly customizable based on individual patient needs. According to the Mayo Clinic, about 9 out of 10 people who get cataract surgery see better afterward, though vision may be blurry at first while the eye recovers.
The most important points to remember include:
- Cataracts develop from multiple causes, such as aging, diabetes, UV exposure, eye trauma, and certain medications.
- Several surgical techniques exist, including phacoemulsification, femtosecond laser-assisted surgery, and manual extracapsular extraction.
- IOL selection directly shapes post-surgical visual outcomes and spectacle dependence.
- Complications like posterior capsule opacification and infection are possible but uncommon and typically treatable.
- Recovery expectations, candidacy criteria, and lens options should all be discussed with your eye care provider before surgery.
Eye Surgery Today provides surgeon-reviewed guides covering each of these topics to support informed decision-making throughout every stage of the cataract surgery process.




