Cataract surgery is a procedure that removes the clouded natural lens and replaces it with an artificial intraocular lens. Major complications occur in fewer than 2% of cases, yet understanding the full risk landscape may help patients make more informed surgical decisions.
This guide covers common postoperative issues, serious but rare surgical risks, intraoperative events, high-risk patient populations, prevention and recovery protocols, warning signs that require urgent attention, and treatment options when complications arise.
Complications such as posterior capsule opacification, dry eye, elevated intraocular pressure, and residual refractive error affect a meaningful number of patients but typically respond well to standard management. PCO alone can develop in up to 54% of cases over time, though a quick laser procedure restores clarity for most.
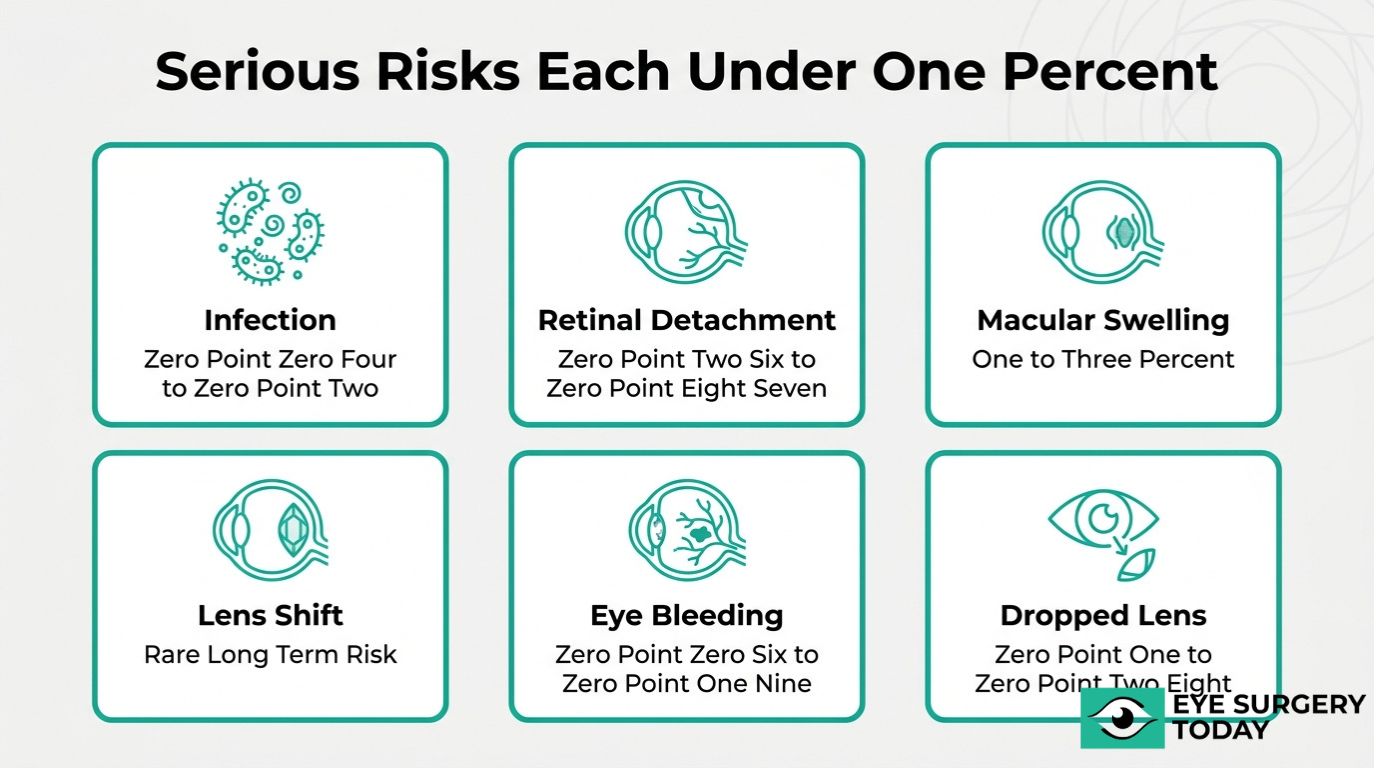
Serious but rare risks, including endophthalmitis, retinal detachment, cystoid macular edema, and suprachoroidal hemorrhage, each occur in well under 1% of procedures. Prompt recognition and treatment are essential because delays with these conditions can threaten long-term vision.
Certain patients face elevated complication rates based on pre-existing conditions. Diabetic patients may experience CME rates as high as 29.5%, while highly myopic eyes carry a significantly greater likelihood of retinal detachment. Glaucoma, prior eye surgery, and dense cataracts each introduce specific anatomical challenges that require tailored surgical planning.
Prevention spans the entire surgical timeline. Preoperative protocols such as povidone-iodine antisepsis and intracameral antibiotics can reduce infection risk, while disciplined postoperative care with prescribed drops and follow-up visits helps catch treatable issues early.
How Common Are Complications From Cataract Surgery?
Complications from cataract surgery are uncommon. Major complications occur in fewer than 2% of cases, making modern cataract surgery one of the safest surgical procedures performed today. According to the AAO Preferred Practice Pattern (2021), the overall rate of serious adverse events remains low when experienced surgeons follow evidence-based protocols. Minor, self-resolving issues such as transient elevated intraocular pressure are more frequent than sight-threatening events, though even these typically respond well to standard postoperative management.
That said, “uncommon” does not mean “impossible.” Certain complications, such as posterior capsule opacification, can develop in a meaningful percentage of patients over time, while rare but serious risks like endophthalmitis and retinal detachment require awareness and prompt action. For patients considering this procedure, understanding the realistic probability of each complication is far more useful than a blanket reassurance that nothing will go wrong.
The sections that follow cover the most common complications, serious but rare risks, intraoperative events, early warning signs, high-risk populations, and prevention strategies to help you prepare with confidence.
What Are the Most Common Complications After Cataract Surgery?
The most common complications after cataract surgery include posterior capsule opacification, dry eye, increased intraocular pressure, residual refractive error, and visual disturbances such as floaters. Each is explored below.
Posterior Capsule Opacification
Posterior capsule opacification (PCO) is the most frequent complication following cataract surgery. Sometimes called “secondary cataract” or “after-cataract,” PCO occurs when residual lens epithelial cells proliferate and migrate across the capsular bag, gradually clouding the membrane behind the intraocular lens implant.
According to the AAO Preferred Practice Pattern (2021) and a 2014 Cochrane review, PCO incidence ranges from 5% to 54% depending on IOL type and follow-up duration. Hydrophobic acrylic lenses with sharp posterior edges tend to inhibit cell migration more effectively, which is why IOL design plays such a significant role in long-term outcomes.
Symptoms typically develop months to years after surgery, causing blurred vision that closely mimics the original cataract. A quick, painless Nd:YAG laser capsulotomy restores clarity in most cases. Because PCO is so common yet so treatable, it deserves attention but rarely warrants concern.
Dry Eye After Cataract Surgery
Dry eye after cataract surgery is one of the most frequently reported postoperative complaints. The corneal incision and exposure to microscope light during the procedure can temporarily disrupt corneal nerve function and reduce tear film stability.
Most patients experience some degree of dryness, grittiness, or fluctuating vision in the weeks following surgery. These symptoms often peak within the first month and gradually improve as corneal nerves regenerate. Preservative-free artificial tears, punctal plugs, and short courses of anti-inflammatory drops can help manage discomfort during recovery.
Patients with pre-existing dry eye disease or those taking medications that reduce tear production may experience more pronounced symptoms. Identifying and treating baseline dry eye before surgery is one of the most underappreciated and important steps in surgical planning, since untreated dryness also affects the accuracy of preoperative lens measurements.
Increased Intraocular Pressure
Increased intraocular pressure (IOP) is a common early complication after cataract surgery. Residual viscoelastic material (OVD), inflammatory debris, or small lens fragments can temporarily obstruct the trabecular meshwork, causing a pressure spike within hours to days of the procedure.
According to the AAO Preferred Practice Pattern (2021), transient IOP elevation is one of the most frequently observed postoperative findings. In most cases, the spike resolves on its own or responds quickly to short-term pressure-lowering drops. Patients with pre-existing glaucoma or pseudoexfoliation syndrome may be more susceptible to sustained elevations, making close early follow-up essential for this group.
Routine postoperative pressure checks allow surgeons to detect and manage IOP spikes before they cause optic nerve damage. Prompt intervention keeps this complication well controlled in the vast majority of patients.
Residual Refractive Error
Residual refractive error is a complication in which the patient’s postoperative prescription does not match the intended visual target. IOL power calculations depend on precise preoperative measurements of corneal curvature, axial length, and anterior chamber depth; small inaccuracies in any variable can shift the outcome.
Modern biometry devices and advanced IOL formulas have significantly improved predictability, yet some patients still require glasses or contact lenses after surgery for fine-tuning. Patients who have undergone prior refractive surgery, such as LASIK or PRK, present a particular challenge because their altered corneal shape complicates standard calculations.
When residual error is clinically significant, options include spectacle correction, laser enhancement procedures, or IOL exchange. Setting realistic expectations before surgery remains the most effective way to ensure patient satisfaction with the visual result.
Floaters and Visual Disturbances
Floaters and visual disturbances after cataract surgery can include new floaters, halos, glare, and dysphotopsia. These symptoms often result from changes in how light interacts with the new intraocular lens or from increased awareness of pre-existing vitreous opacities once the cloudy natural lens has been removed.
Positive dysphotopsia (glare or halos) and negative dysphotopsia (a temporal crescent shadow) are related to IOL edge design and typically diminish as the brain adapts over several weeks. New-onset floaters alone are usually benign, but a sudden increase in floaters accompanied by flashes of light warrants urgent evaluation to rule out retinal tear or detachment.
Most visual disturbances improve with neuroadaptation during the first three months. Understanding which symptoms are expected and which signal a serious complication helps patients respond appropriately during recovery.
What Are the Serious but Rare Risks of Cataract Surgery?
The serious but rare risks of cataract surgery include endophthalmitis, retinal detachment, cystoid macular edema, dislocated intraocular lens, suprachoroidal hemorrhage, and dropped nucleus.
Endophthalmitis
Endophthalmitis is a severe intraocular infection that can occur after cataract surgery. Bacteria, most commonly Staphylococcus epidermidis, may enter the eye during or shortly after the procedure, triggering intense inflammation. Symptoms typically appear within days to weeks and can include sudden pain, redness, and rapid vision loss. Although the incidence in the United States ranges from approximately 0.04% to 0.2%, endophthalmitis remains one of the most feared postoperative complications because delayed treatment can result in permanent vision damage. Preoperative antisepsis with povidone-iodine and intracameral antibiotics have significantly reduced its occurrence. Endophthalmitis prevention protocols represent one of the clearest success stories in modern cataract surgery, making surgeon adherence to these steps critical.
Retinal Detachment
Retinal detachment is a separation of the neurosensory retina from the retinal pigment epithelium, often associated with vitreous traction or tears following cataract surgery. According to the AAO Preferred Practice Pattern (2021) and Stein et al. (2011), the incidence ranges from 0.26% to 0.87%, though long-term risk may reach up to 4% in certain populations. This complication typically develops months to years after surgery rather than in the immediate postoperative period. Warning signs include sudden flashes of light, a shower of new floaters, or a shadow encroaching on peripheral vision. Because retinal detachment can cause irreversible vision loss without prompt surgical repair, any of these symptoms warrants urgent evaluation by an ophthalmologist.
Cystoid Macular Edema
Cystoid macular edema is fluid accumulation in the macula caused by inflammatory mediators released after cataract surgery. Also known as Irvine-Gass Syndrome, clinically significant CME affects approximately 1% to 3% of patients, typically appearing four to six weeks postoperatively. According to the PREMED Study (2018), prophylactic topical NSAIDs combined with corticosteroids can reduce the incidence, particularly in higher-risk groups. Blurred or distorted central vision is the hallmark symptom. While most cases resolve with anti-inflammatory treatment, recalcitrant CME may require intravitreal steroid or anti-VEGF injections. For patients with diabetes or uveitis, proactive management of macular edema risk is especially important since these groups face substantially elevated rates.
Dislocated Intraocular Lens
A dislocated intraocular lens is a shift or displacement of the implanted IOL from its intended position within the capsular bag. This complication may occur early due to insufficient capsular support or years later as the zonular fibers gradually weaken. Symptoms can include blurred vision, double vision, or visible edge glare from the shifted lens. Depending on severity, treatment options range from IOL repositioning and scleral fixation to complete IOL exchange. Patients with pseudoexfoliation syndrome or a history of ocular trauma face a higher likelihood of late dislocation, making long-term monitoring especially valuable for these individuals.
Suprachoroidal Hemorrhage
Suprachoroidal hemorrhage is bleeding into the suprachoroidal space, often triggered by sudden intraoperative hypotony. According to the AAO Preferred Practice Pattern (2021), this complication occurs in approximately 0.06% to 0.19% of cataract procedures. Although extremely rare, it can be sight-threatening when severe. Risk factors include advanced age, anticoagulant use, glaucoma, and elevated blood pressure. Intraoperative recognition and prompt wound closure are essential to limit its progression. Among all intraoperative complications, suprachoroidal hemorrhage is one that underscores the importance of thorough preoperative medical examination.
Dropped Nucleus
A dropped nucleus is the descent of lens material into the vitreous cavity, typically following a posterior capsule rupture during phacoemulsification. This complication occurs in approximately 0.1% to 0.28% of cases and usually requires a secondary procedure, pars plana vitrectomy, to retrieve the retained lens fragments. Leaving nuclear material in the vitreous may lead to chronic inflammation, elevated intraocular pressure, or retinal detachment. Dense or mature cataracts increase the risk because they require higher phacoemulsification energy. When managed promptly by a vitreoretinal specialist, visual outcomes can still be favorable despite the added complexity.
Understanding these rare but serious risks helps guide informed conversations with your surgeon about individualized prevention strategies.
What Complications Can Happen During Cataract Surgery?
Complications during cataract surgery are intraoperative events that may affect the surgical outcome. The three most commonly emphasized intraoperative concerns include posterior capsule tear, zonular dehiscence, and corneal wound complications.
What Is a Posterior Capsule Tear?
A posterior capsule tear is a rupture of the thin membrane that holds the natural lens in place, potentially leading to vitreous prolapse into the anterior chamber. This complication occurs during the phacoemulsification process when excessive pressure or surgical maneuvers compromise the capsule’s integrity.
According to the AAO Preferred Practice Pattern (2021) and Jaycock et al. (2009), posterior capsule tear with vitreous loss occurs in approximately 1.5% to 3.5% of cases, with low-risk patients averaging around 2%. When vitreous enters the anterior chamber, the surgeon must perform an anterior vitrectomy before proceeding with intraocular lens placement.
Patients with dense cataracts or prior eye surgery face elevated risk for this complication. Early recognition during the procedure allows the surgical team to adjust technique and minimize downstream consequences for visual recovery.
What Happens if There Is Zonular Dehiscence?
Zonular dehiscence is a weakening or separation of the zonular fibers that suspend the lens capsule within the eye. These fibers anchor the capsular bag to the ciliary body, and when they fail, the lens can become unstable or dislocate during surgery.
Certain conditions significantly increase this risk. According to the AAO Preferred Practice Pattern (2021), patients with pseudoexfoliation syndrome or glaucoma face an increase in the risk of capsular tear and zonular dehiscence and independent studies show that a relatively shallow anterior chamber in these patients is associated with a greater likelihood of surgical difficulty and complications compared with eyes with deeper chambers. Small pupils and weak zonules compound the difficulty of safe lens removal.
When a surgeon identifies zonular instability, capsular tension rings or specialized hooks can stabilize the bag. In clinical practice, thorough preoperative assessment of zonular integrity remains one of the most effective ways to anticipate and manage this challenge.
How Can Corneal Wound Complications Occur Intraoperatively?
Corneal wound complications can occur intraoperatively when the surgical incision in the cornea becomes compromised during the procedure. The small incisions created for phacoemulsification may develop issues, such as:
- Wound leakage from an improperly constructed or thermally damaged incision
- Descemet membrane detachment caused by instrument entry through the corneal layers
- Corneal burns from excessive ultrasound energy delivered near the wound site
These complications may result from tissue characteristics that make incision architecture less predictable, including thin corneas or prior corneal surgery. Precise wound construction at the appropriate depth and length helps maintain anterior chamber stability throughout the procedure.
Surgeons who identify wound instability intraoperatively can place sutures to secure the incision. Recognizing these intraoperative risks highlights why postoperative monitoring remains equally important for detecting delayed healing issues.
What Are the Early Warning Signs of a Complication After Cataract Surgery?
The early warning signs of a complication after cataract surgery include sudden vision loss, increasing eye pain, new flashes or floaters, worsening redness, and light sensitivity that intensifies rather than improves. While mild discomfort and slight blurriness are normal during the first few days of recovery, symptoms that escalate or appear suddenly may indicate a serious postoperative problem requiring immediate attention.
Recognizing these signs early can be the difference between a straightforward treatment and a vision-threatening outcome. The following symptoms, when they appear in the days or weeks after surgery, should prompt an urgent call to your ophthalmologist:
- Sudden or severe vision decrease may signal endophthalmitis, retinal detachment, or cystoid macular edema.
- Increasing eye pain that does not respond to prescribed drops can indicate infection or elevated intraocular pressure.
- New flashes of light or a sudden increase in floaters may suggest retinal traction or detachment, which can develop months after the procedure.
- Progressive redness or swelling around the eye, particularly with discharge, may point toward an inflammatory or infectious process.
- A shadow or curtain effect across part of the visual field is a hallmark warning sign of retinal detachment.
- Sensitivity to light that worsens over time, rather than gradually improving, can reflect intraocular inflammation such as Irvine-Gass Syndrome.
According to the AAO Preferred Practice Pattern (2021), red flags after cataract surgery include pain, sudden vision loss, and flashes or floaters, all of which warrant same-day evaluation by the treating surgeon.
Most of these warning signs overlap with conditions that range widely in severity. A transient pressure spike, for example, may resolve with a single office visit, while untreated endophthalmitis can lead to permanent vision loss within days. The critical factor is timing: any new or worsening symptom in and after the initial recovery window deserves professional evaluation rather than a wait-and-see approach. In clinical practice, patients who contact their surgeon early almost always have better outcomes than those who delay.
Understanding who faces elevated risk for these complications helps put warning signs into proper context.
Who May Be at Higher Risk for Cataract Surgery Complications?
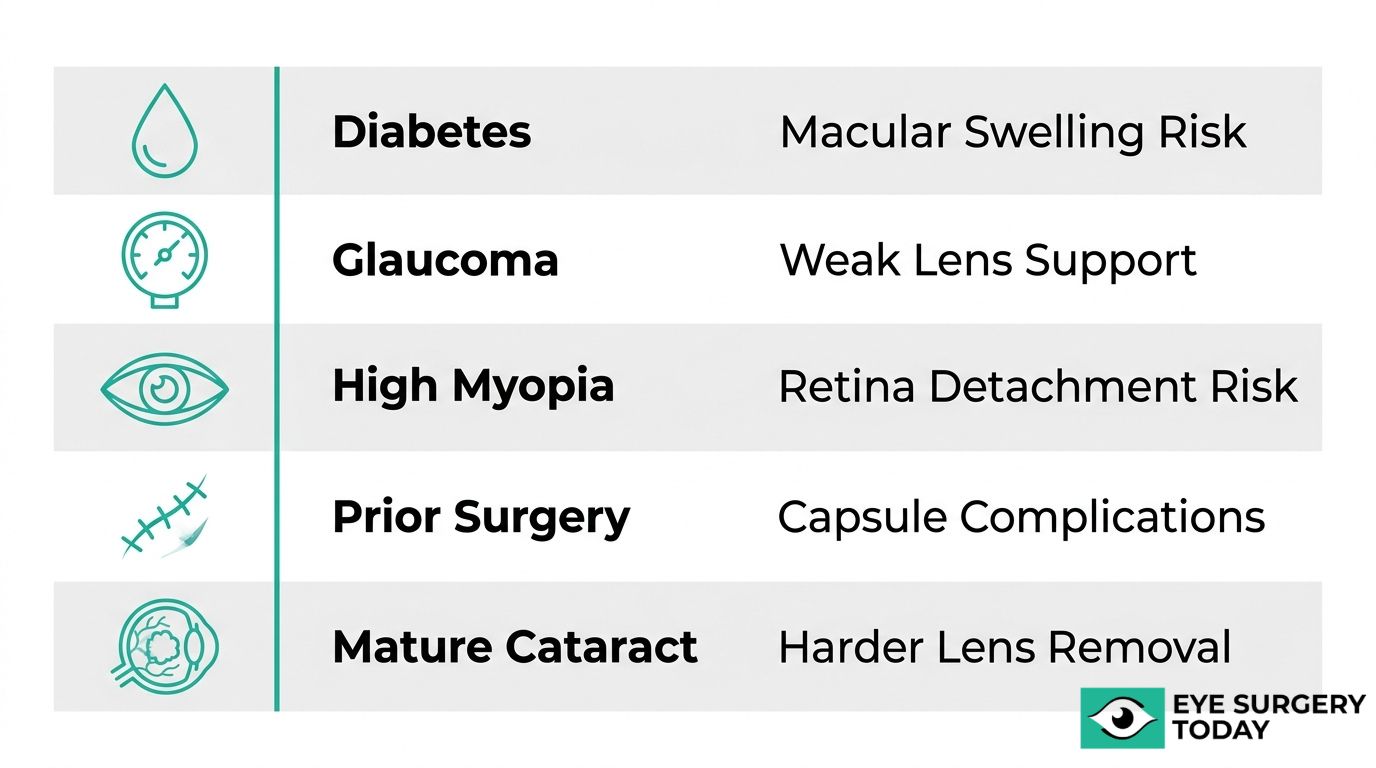
Patients with diabetes, glaucoma, high myopia, previous eye surgery, or mature cataracts may face higher complication risks. The following sections cover each high-risk group and its specific concerns.
What Risks Do Patients With Diabetes Face?
Patients with diabetes face elevated risks for cystoid macular edema and postoperative infection after cataract surgery. Diabetic retinopathy and impaired wound healing are the primary contributing factors.
According to the 2018 PREMED study and the AAO Preferred Practice Pattern (2021), CME rates may reach up to 29.5% in diabetic patients, while endophthalmitis risk increases with an odds ratio of approximately 1.3 to 1.5 compared to non-diabetic individuals.
Prophylactic topical NSAIDs combined with corticosteroids can help reduce CME risk in this population. Because diabetic patients often experience slower and less predictable healing, their recovery timelines may differ from standard expectations. Thorough preoperative assessment of retinopathy status is one of the most important steps a surgeon can take to anticipate and mitigate these risks.
How Does Glaucoma Affect Complication Risk?
Glaucoma affects complication risk by introducing anatomical challenges, such as small pupils and weakened zonules, that make cataract surgery technically more demanding. Pseudoexfoliation syndrome, commonly associated with glaucoma, further compromises zonular integrity.
According to the AAO Preferred Practice Pattern (2021), patients with a more shallow anterior chamber depth may face an increase in the risk of capsular tear or zonular dehiscence. These structural vulnerabilities can complicate lens removal and intraocular lens placement. Careful preoperative evaluation of anterior segment anatomy helps surgeons plan for iris expansion devices or capsular tension rings when needed.
What Are the Risks for Patients With High Myopia?
The risks for patients with high myopia center primarily on a significantly elevated rate of retinal detachment after cataract surgery. Eyes with an axial length greater than 26mm have inherently thinner peripheral retinas and increased vitreous traction.
According to the AAO Preferred Practice Pattern (2021) and Stein et al. (2011), highly myopic eyes have a higher odds of retinal detachment after cataract surgery compared to emmetropic eyes. This makes retinal detachment the single most critical postoperative concern for this group. Long-term monitoring with dilated fundus exams is essential, and patients should be counseled to report flashes, floaters, or curtain-like vision changes immediately.
How Does Previous Eye Surgery Increase Risk?
Previous eye surgery increases risk because prior procedures, such as pars plana vitrectomy, can weaken the zonular fibers that support the lens capsule. This zonular instability makes capsular complications more likely during phacoemulsification.
Capsular tear rates may reach up to 9% in patients with prior vitreoretinal surgery, compared to approximately 2% in low-risk eyes. Surgeons often use capsular tension rings or modified surgical techniques to stabilize the bag in these cases. A detailed surgical history is a highly important element of cataract preoperative planning.
What Complications Are More Likely With Mature or Dense Cataracts?
The complications more likely with mature or dense cataracts include posterior capsule rupture and related intraoperative events. Brunescent nuclei require significantly more phacoemulsification energy to break apart, which increases mechanical stress on the capsule.
According to the AAO Preferred Practice Pattern (2021), poor red reflex visualization in dense cataracts further complicates the procedure by limiting the surgeon’s view of capsular integrity during lens removal. Capsular dye and femtosecond laser-assisted capsulotomy can help improve safety in these challenging cases. Patients with long-delayed cataract surgery should understand that earlier intervention, when the lens is softer, generally allows for a smoother procedure.
Understanding individual risk factors helps both patients and surgeons plan for safer outcomes and more targeted prevention strategies.
How Can You Help Prevent Complications Before Cataract Surgery?
You can help prevent complications before cataract surgery by following preoperative protocols that reduce infection risk, manage existing conditions, and prepare the eye for a safer procedure.
Preoperative prevention starts with thorough communication between patient and surgeon. Your ophthalmologist may recommend specific steps based on your individual risk profile, including medication adjustments and targeted eye treatments. According to the AAO Preferred Practice Pattern (2021), meticulous preoperative planning is essential because the ophthalmologist must confirm the cataract, determine surgical need, and design a treatment plan that accounts for potential complications.
Several key prevention strategies can reduce your risk before the procedure takes place:
- Disclose your full medication list. Alpha-blockers such as tamsulosin (Flomax) are associated with intraoperative floppy iris syndrome (IFIS), and your surgeon needs this information to plan accordingly.
- Manage diabetes and blood sugar levels. Diabetic patients face elevated risks for cystoid macular edema and endophthalmitis, so stabilizing glucose before surgery may help reduce these complications.
- Follow antiseptic protocols on surgery day. Povidone-iodine antisepsis (5% solution applied for 3 minutes) is the gold standard for reducing endophthalmitis risk.
- Address existing eye conditions. Glaucoma, pseudoexfoliation syndrome, and prior eye surgeries can weaken zonular support, increasing the chance of capsular tears during the procedure.
- Attend all preoperative assessments. Biometry measurements and anterior chamber depth evaluation help your surgeon identify structural risk factors, such as shallow anterior chambers that may carry an increase in capsular tear risk.
Patients with dense or mature cataracts should discuss surgical approach options with their surgeon, since brunescent nuclei require higher phaco energy and present reduced visualization during surgery. In clinical practice, the preoperative consultation is often the single most impactful opportunity to reduce surgical risk, because it allows the surgeon to tailor technique, IOL selection, and prophylactic medications to each patient’s unique anatomy. Understanding what happens after the procedure is equally important for a safe recovery.
What Should You Do After Surgery to Reduce Complication Risk?
After surgery, you should follow your ophthalmologist’s postoperative care plan closely to reduce complication risk. Key steps include using prescribed eye drops, protecting the eye, and attending all follow-up appointments.
Proper postoperative behavior directly influences healing outcomes. Your surgeon may prescribe a regimen of antibiotic and anti-inflammatory eye drops to prevent infection and control swelling. As noted in the AAO Preferred Practice Pattern (2021), meticulous postoperative care is a core component of the treatment plan designed to manage potential complications.
During the first few weeks, patients can lower their risk by following these guidelines:
- Use prescribed antibiotic drops exactly as directed to reduce endophthalmitis risk.
- Apply anti-inflammatory drops, such as topical NSAIDs or corticosteroids, to help prevent cystoid macular edema.
- Wear the protective eye shield while sleeping, especially during the first week.
- Avoid rubbing or pressing on the operated eye.
- Refrain from heavy lifting, bending at the waist, and strenuous exercise for the period your surgeon specifies.
- Keep water, soap, and dust away from the eye during the initial healing phase.
- Attend every scheduled follow-up visit so your surgeon can monitor intraocular pressure and check for early signs of inflammation or infection.
Missing even a single follow-up appointment can delay detection of treatable issues like elevated intraocular pressure or early macular edema. In clinical practice, the patients who recover most smoothly are those who treat the postoperative drop schedule with the same seriousness as the surgery itself.
When Should You Contact Your Eye Surgeon After Cataract Surgery?
You should contact your eye surgeon after cataract surgery whenever you notice sudden changes in vision, increasing pain, or new symptoms that fall outside normal recovery expectations. The warning signs below require prompt evaluation.
Contact your eye surgeon immediately if you experience any of the following:
- Sudden vision loss or a noticeable decrease in clarity that does not improve within hours.
- Increasing eye pain that worsens despite prescribed medications.
- New flashes of light or a sudden increase in floaters, which may indicate retinal detachment or other vitreous complications.
- Redness that worsens rather than improves after the first few days, as this can signal endophthalmitis or severe inflammation.
- Sensitivity to light combined with deep, aching pain, particularly within the first week.
- A shadow or curtain effect across any part of your visual field.
Some of these symptoms, particularly flashes and floaters appearing weeks to months after surgery, may point to retinal detachment, which the AAO Preferred Practice Pattern (2021) identifies as occurring in approximately 0.2% to 1% of cases postoperatively. Although rare, delayed recognition can compromise visual outcomes.
Mild discomfort, slight grittiness, and minor fluctuations in vision are expected during the first few days of recovery. However, any symptom that feels distinctly different from what your surgeon described as normal warrants a call. In clinical practice, the threshold for contacting your surgeon should always be low; a brief phone consultation costs nothing, while delayed treatment of a genuine complication can be far more difficult to solve.
Understanding when to seek help is one step; knowing how complications are actually treated provides further reassurance.
How Are Cataract Surgery Complications Treated if They Occur?
Cataract surgery complications are treated with targeted interventions that range from quick outpatient laser procedures to surgical correction. The following subsections cover treatments for PCO, infection, macular edema, and IOL dislocation.
How Is Posterior Capsule Opacification Treated?
Posterior capsule opacification is treated with Nd:YAG laser capsulotomy, a quick, noninvasive outpatient procedure. During capsulotomy, the ophthalmologist uses a focused laser beam to create an opening in the clouded posterior capsule, restoring a clear visual axis. The procedure typically takes only a few minutes and requires no incision or anesthesia beyond dilating drops.
Vision improvement is usually noticeable within hours to days. Because PCO can develop months to years after the original cataract surgery, patients sometimes mistake the gradual blurring for a new cataract forming. YAG capsulotomy remains one of the most frequently performed laser procedures in ophthalmology, and its low complication profile makes it a reliable solution for what is sometimes called “secondary cataract.”
How Is Post-Surgical Infection Managed?
Post-surgical infection, specifically endophthalmitis, is managed as an ophthalmic emergency requiring immediate intervention. The standard first-line treatment involves an intravitreal tap and injection of antibiotics, typically vancomycin combined with ceftazidime or amikacin, delivered directly into the vitreous cavity.
If the patient’s vision has declined to light perception or worse, the ophthalmologist may recommend pars plana vitrectomy to remove infected vitreous material and improve antibiotic penetration. Early detection is critical; even a few hours of delay can significantly affect visual outcomes. Endophthalmitis occurs in approximately 0.04% to 0.2% of cataract surgeries in the United States, yet according to the AAO Preferred Practice Pattern (2021), its potential severity demands aggressive, time-sensitive treatment whenever it arises.
What Treatment Options Exist for Cystoid Macular Edema?
The treatment options for cystoid macular edema include topical anti-inflammatory medications as the initial approach, with escalating therapies reserved for persistent cases. Ophthalmologists typically prescribe a combination of topical NSAIDs and corticosteroid eye drops to reduce the inflammatory mediators responsible for fluid accumulation in the macula.
When CME proves recalcitrant and does not respond to topical therapy, intravitreal injections of corticosteroids or anti-VEGF agents may be considered. Most cases of post-cataract CME, also known as Irvine-Gass syndrome, improve with treatment and resolve over several weeks to months of consistent treatment. For patients with diabetes, whose CME risk can be substantially elevated, closer monitoring and earlier escalation to intravitreal therapy may be warranted. Timely intervention typically preserves visual acuity in the majority of affected patients.
How Is a Dislocated Intraocular Lens Corrected?
A dislocated intraocular lens is corrected through surgical intervention, with the specific approach depending on the severity and direction of displacement. The three primary options are IOL repositioning, scleral fixation, and IOL exchange.
- IOL repositioning involves surgically returning the displaced lens implant to its proper alignment within the capsular bag or sulcus.
- Scleral fixation sutures or secures the IOL to the scleral wall when the capsular support structure is insufficient to hold the lens.
- IOL exchange removes the original implant entirely and replaces it with a new lens designed for alternative fixation.
Mild subluxation may sometimes be monitored if the patient remains asymptomatic, though progressive displacement generally requires surgical correction. In clinical practice, the choice between these techniques depends on how much capsular bag integrity remains, making a thorough intraoperative assessment essential.
With effective treatments available for each complication, understanding your surgical options can help you approach cataract surgery with greater confidence.
How Can a Surgeon-Led Educational Platform Help You Prepare for Cataract Surgery?
A surgeon-led educational platform can help you prepare for cataract surgery by providing clinically accurate, easy-to-understand information about risks, prevention, and recovery expectations. This comprehensive understanding can alleviate concerns, reinforcing why modern cataract surgery is pain-free and safe for the vast majority of patients.
Can Eye Surgery Today’s Expert Guides Help You Understand Your Surgical Risks?
Yes, Eye Surgery Today’s expert guides can help you understand your surgical risks by translating complex clinical data into clear, patient-focused language. The platform was founded by nationally recognized ophthalmology key opinion leaders specifically to bridge the gap between surgical expertise and patient understanding.
Eye Surgery Today covers the full spectrum of cataract surgery topics, including:
- Complication types, from common issues like posterior capsule opacification to rare events like endophthalmitis
- Risk factors specific to conditions such as diabetes, glaucoma, and high myopia
- Prevention strategies grounded in current clinical guidelines
- Recovery expectations and warning signs that require prompt medical attention
Because practicing surgeons review every guide, the information reflects real-world clinical experience rather than generalized health content. For patients weighing whether to proceed with surgery, this level of transparency can make the difference between informed confidence and unnecessary anxiety.
What Are the Key Takeaways About Cataract Surgery Complications and Prevention?
The key takeaways about cataract surgery complications and prevention are that serious complications remain rare, most risks are manageable with proper planning, and informed patients can be more confident in their decisions. Large datasets support low overall complication rates, with most individual serious complications occurring at around <1–2% each.
The most actionable lessons from this guide include:
- Not all complications carry equal weight; common issues like temporary dry eye differ significantly from rare events like retinal detachment
- Pre-existing conditions, particularly diabetes, glaucoma, and high myopia, influence individual risk profiles
- Proven prevention protocols, such as antisepsis techniques and prophylactic medications, substantially reduce infection and inflammation rates
- Recognizing early warning signs after surgery allows faster intervention and better visual outcomes
- Choosing a surgeon who prioritizes thorough preoperative evaluation and patient education is one of the most effective steps any patient can take
Understanding both the risks and the safeguards gives patients a realistic foundation for surgical decision-making, rather than relying on incomplete information.





