Refractive vision correction is a category of surgical procedures that reshape or bypass the eye’s optical imperfections to reduce or eliminate dependence on glasses and contact lenses. These procedures correct refractive errors, which occur when the eye’s shape prevents light from focusing properly on the retina.
This guide covers the refractive errors these procedures treat, the major surgical options available, how each procedure compares for different patient profiles, candidacy and risk considerations, and the practical factors of recovery and cost.
Myopia, hyperopia, astigmatism, and presbyopia each affect light focus differently, and specific procedures target each condition through distinct mechanisms. LASIK, PRK, SMILE, ICL, and refractive lens exchange represent the primary approaches, ranging from corneal reshaping with excimer and femtosecond lasers to implanting phakic intraocular lenses or replacing the natural lens entirely.
Choosing the right procedure depends on individual anatomy. Corneal thickness, prescription strength, age, and conditions like dry eye or keratoconus all influence which option may be most appropriate. PRK may suit thinner corneas where flap creation poses risk, while ICL can address high myopia that falls outside laser correction thresholds.
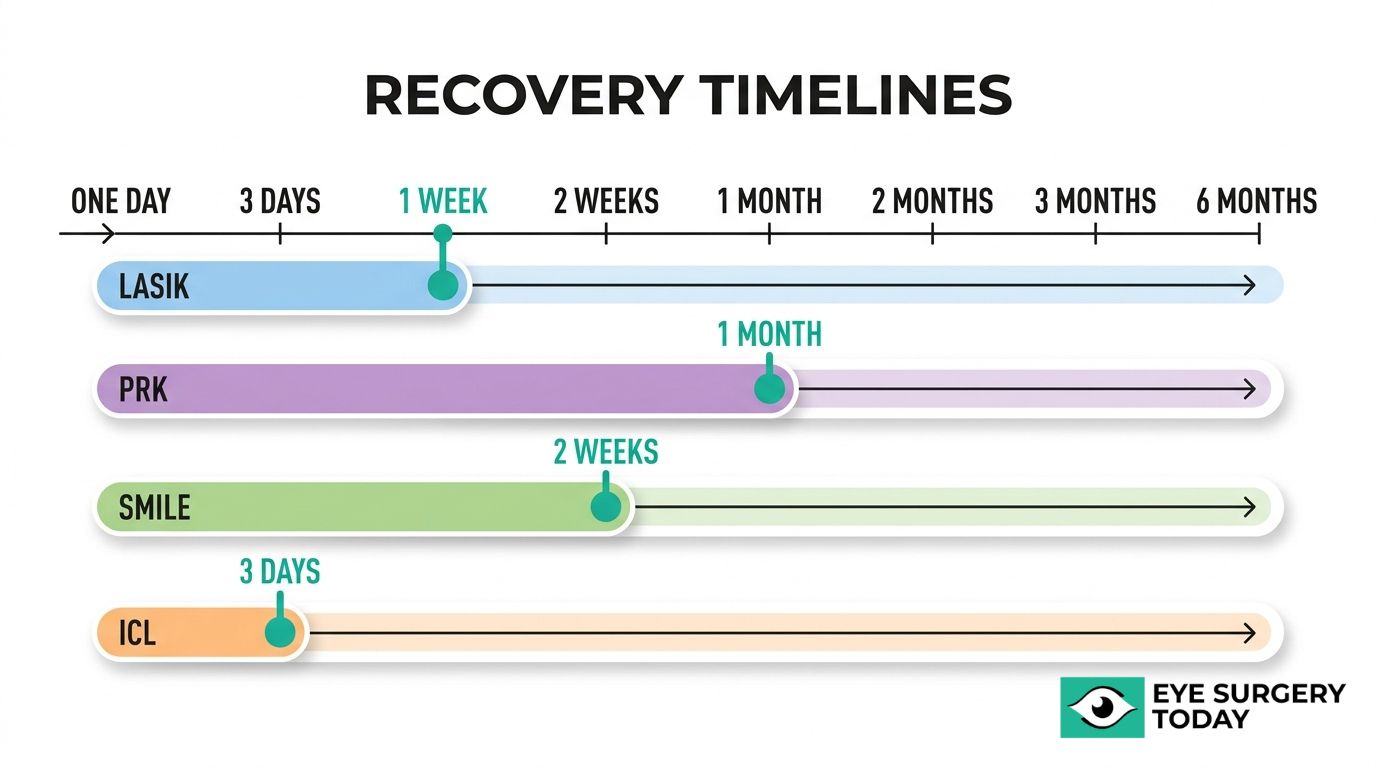
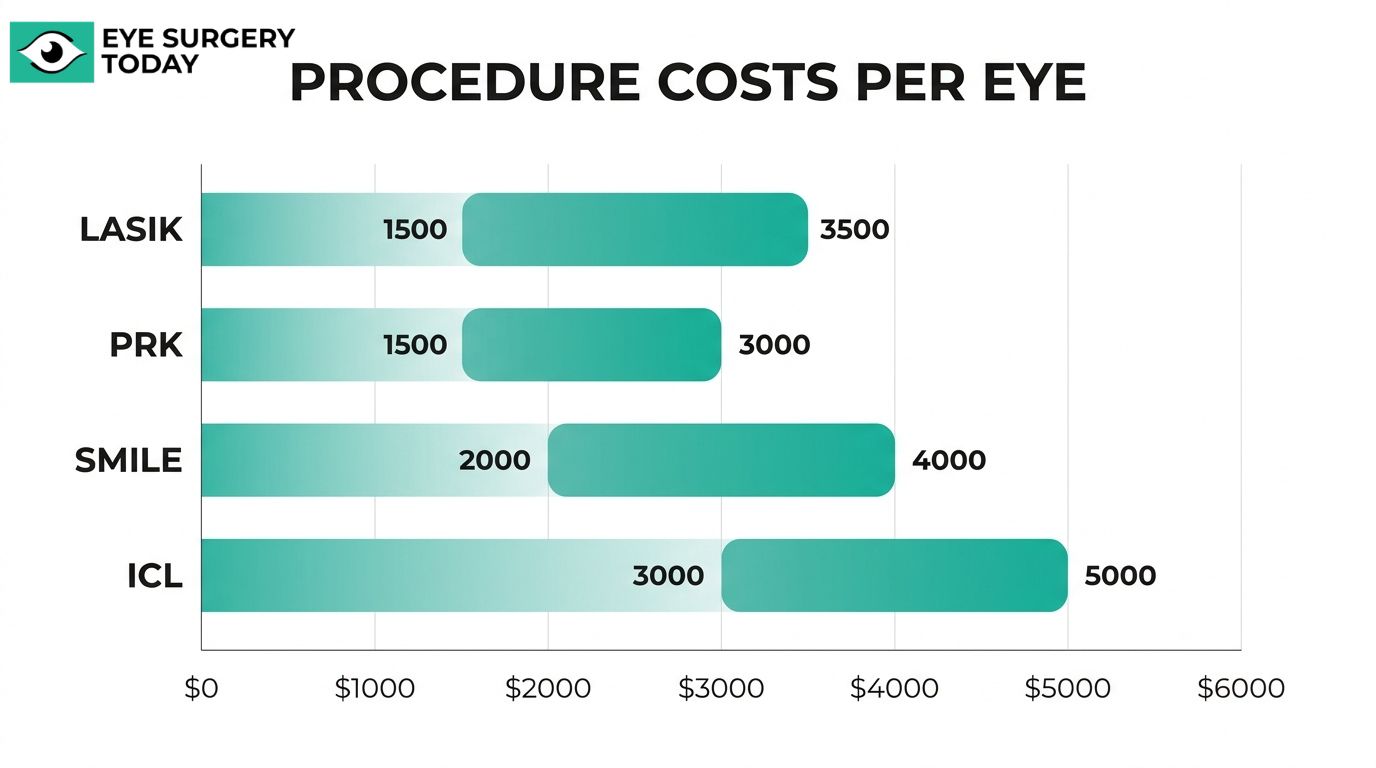
Each procedure carries a different risk profile, recovery timeline, and cost range. LASIK recovery may begin within hours; PRK requires days of epithelial regeneration; ICL typically allows rapid visual improvement within a day or two. Costs range from approximately $1,500 per eye for surface procedures to $5,000 or more for lens-based options.
Understanding these differences, along with the right questions to ask a surgeon, can help match the right procedure to your specific visual needs and goals.
What Is Refractive Vision Correction?
Refractive vision correction is a category of surgical procedures that reshape the eye’s optical system to reduce or eliminate dependence on glasses and contact lenses. These procedures correct refractive errors, which occur when the eye’s shape prevents light from focusing properly on the retina. The following sections explain how refractive errors develop and which conditions these procedures can treat.
What Refractive Errors Can Vision Correction Procedures Treat?
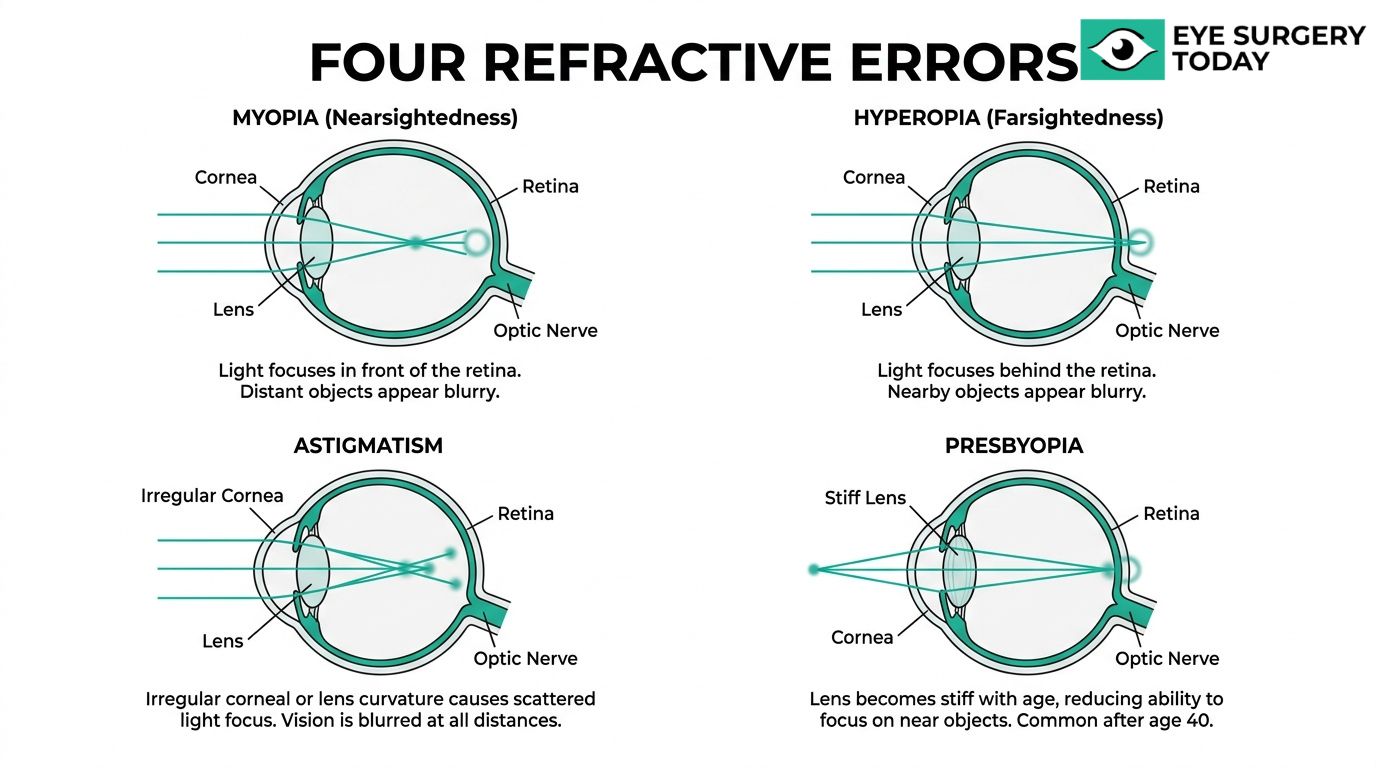
Vision correction procedures can treat four primary refractive errors: myopia, hyperopia, astigmatism, and presbyopia. Each condition affects how light focuses on the retina, and specific procedures target each one differently.
Myopia (Nearsightedness)
Myopia is a refractive error that occurs when the eyeball grows too long or the cornea is too curved, causing distant objects to appear blurry while close objects remain clear. According to the National Eye Institute, this misfocused light falls in front of the retina rather than directly on it.
Several vision correction procedures can treat myopia:
- LASIK reshapes the cornea to flatten its curvature.
- PRK removes surface corneal tissue to achieve a similar correction.
- SMILE extracts a small lenticule from within the cornea.
- ICL implants a lens inside the eye for moderate to high myopia.
For patients with high myopia, thin corneas, or severe dry eyes, ICL may be an excellent option when laser vision correction is not suitable. The rising prevalence of myopia makes understanding these treatment pathways increasingly relevant for prospective patients.
Hyperopia (Farsightedness)
Hyperopia is a refractive error that occurs when the eyeball is too short or the cornea is too flat, causing near objects to appear blurry while distant objects may remain clearer. Light focuses behind the retina instead of on it, which can also strain the eyes during close-up tasks.
Corrective procedures for hyperopia include:
- LASIK, which steepens the central cornea to improve near focusing.
- PRK, which offers a similar reshaping approach without creating a corneal flap.
- Refractive Lens Exchange, which replaces the natural lens with an artificial intraocular lens for high hyperopia.
- Conductive Keratoplasty, which uses radiofrequency energy to steepen the cornea for low hyperopia.
Not every procedure suits every degree of hyperopia. Higher prescriptions often require lens-based approaches rather than corneal reshaping alone, making a thorough evaluation essential.
Astigmatism
Astigmatism is a refractive error caused by an irregularly shaped cornea or lens, which prevents light from focusing evenly on the retina. This uneven focus can produce blurred or distorted vision at all distances.
Procedures that can correct astigmatism include:
- LASIK, which reshapes the cornea to create a more uniform curvature.
- PRK, often preferred for thinner or more irregular corneas where a flap might be contraindicated.
- SMILE, which corrects the irregularity through a minimally invasive lenticule extraction.
- ICL with toric lens designs, which compensates for astigmatism inside the eye.
Astigmatism frequently occurs alongside myopia or hyperopia rather than in isolation. Because of this overlap, surgeons often address astigmatism simultaneously during a primary refractive procedure.
Presbyopia
Presbyopia is an age-related condition that progressively reduces the eye’s ability to focus on close objects. According to a StatPearls review published through the NCBI Bookshelf, presbyopia affects nearly all adults older than 40.
Unlike myopia, hyperopia, and astigmatism, presbyopia results from the natural lens losing flexibility rather than from corneal shape. Treatment options include:
- Refractive Lens Exchange, which replaces the stiffened natural lens with a multifocal or trifocal intraocular lens.
- Monovision LASIK, which corrects one eye for distance and the other for near vision.
- Conductive Keratoplasty, which can temporarily steepen the cornea for improved near focus.
Presbyopia remains one of the more complex refractive errors to address because it involves the lens rather than the cornea. Patients over 40 exploring refractive surgery should discuss presbyopia management as part of their overall treatment plan, since correcting distance vision alone may still leave near-vision challenges unresolved.
With a clear understanding of each refractive error, the next step is exploring which specific procedures address them.
What Are the Types of Refractive Vision Correction Procedures?
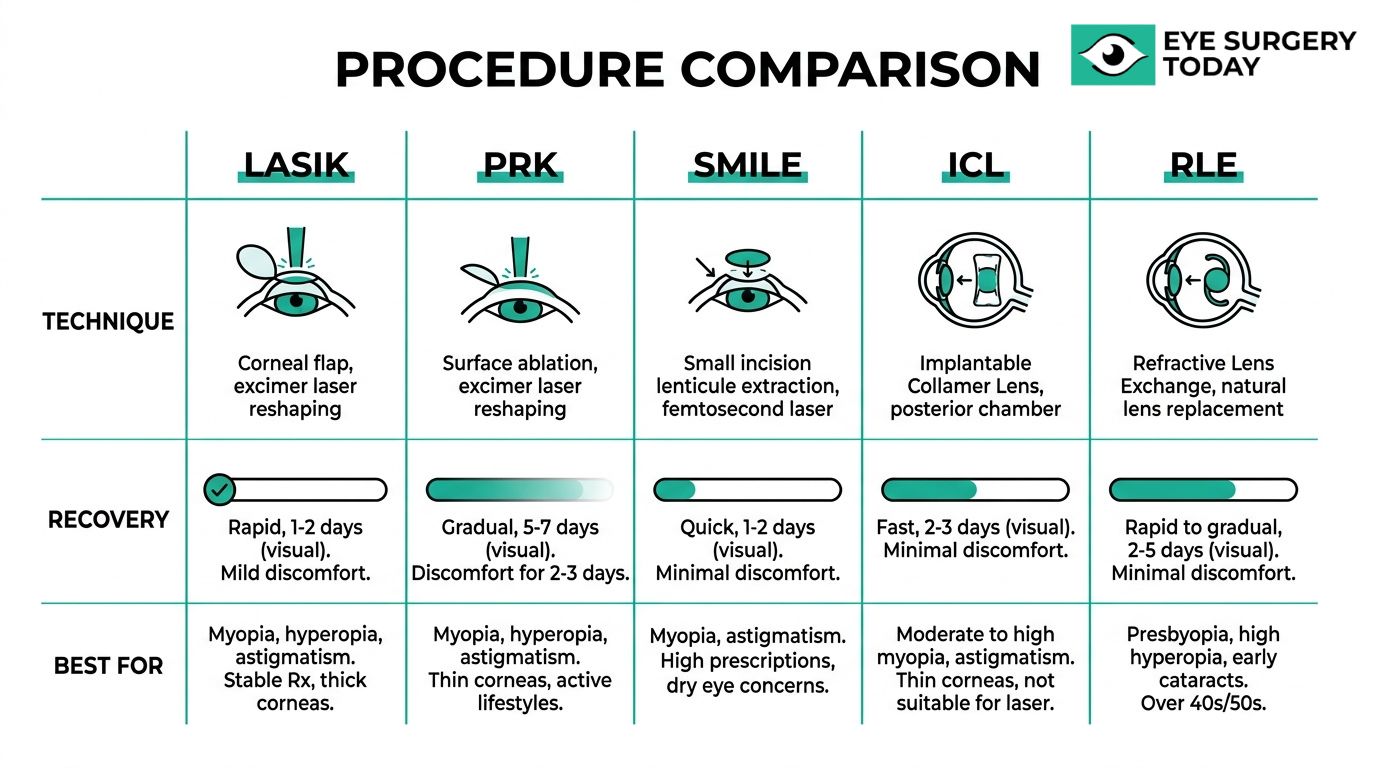
The types of refractive vision correction procedures include LASIK, PRK, SMILE, ICL, refractive lens exchange, and conductive keratoplasty. Each approach reshapes or bypasses optical imperfections through a different mechanism.
LASIK
LASIK is a laser-based refractive procedure that reshapes the corneal stroma to correct myopia, hyperopia, and astigmatism. A surgeon creates a thin corneal flap using a femtosecond laser, then applies an excimer laser to precisely remove tissue from the underlying stroma. The flap is repositioned without stitches, and the reshaped cornea redirects light onto the retina more accurately. Because the surface epithelium remains largely intact under the flap, visual recovery tends to be rapid. Most patients notice clearer vision within 24 hours. LASIK remains the most widely performed refractive procedure, and for good reason: its combination of fast recovery and predictable outcomes makes it the benchmark against which newer options are measured.
PRK (Photorefractive Keratectomy)
PRK is a surface ablation procedure that uses an excimer laser to reshape the cornea after the outer epithelial layer is removed. Unlike LASIK, PRK creates no corneal flap. The excimer laser sculpts the exposed stromal surface directly, correcting myopia, hyperopia, and astigmatism. A bandage contact lens protects the eye while the epithelium regenerates over several days. Recovery takes longer than LASIK, and mild discomfort is common during the first week. PRK may be particularly well suited for patients with thinner or more irregular corneas where flap creation could pose additional risk. Although visual results after full healing are comparable to LASIK, the extended stabilization period is an important factor to discuss with your eye care provider.
SMILE (Small Incision Lenticule Extraction)
SMILE is a flapless, minimally invasive refractive procedure primarily used to correct myopia. According to the American Academy of Ophthalmology, a femtosecond laser creates a small, disc-shaped lenticule within the intact cornea, which the surgeon then extracts through a small incision. Preserving the corneal surface without a flap may reduce dry eye symptoms and improve biomechanical stability compared to flap-based methods. SMILE requires no excimer laser; the femtosecond laser performs the entire correction. For patients concerned about flap-related complications, this flapless approach offers a compelling alternative with a straightforward recovery.
ICL (Implantable Collamer Lens)
ICL surgery involves implanting a phakic intraocular lens inside the eye, positioned behind the iris and in front of the natural lens. This additive approach corrects moderate to high myopia and astigmatism without removing any corneal tissue. The Collamer material is biocompatible and includes UV-filtering properties. Because the natural lens remains untouched, the procedure is considered reversible; the ICL can be removed or exchanged if needed. ICL may be an excellent option for patients whose corneas are too thin for laser-based procedures or who have severe dry eyes. From a clinical standpoint, ICL fills an important gap for high-prescription patients who would otherwise have limited surgical options.
Refractive Lens Exchange
Refractive lens exchange is an elective procedure where the eye’s natural crystalline lens is replaced with an artificial intraocular lens. According to the American Academy of Ophthalmology, RLE (also known as clear lens extraction) may correct high hyperopia or presbyopia. The surgical technique mirrors cataract surgery, though the lens being replaced is clear rather than clouded. Surgeons can select from monofocal, multifocal, or extended-depth-of-focus IOLs to match the patient’s visual goals. RLE is often considered for patients over 40 who are not ideal candidates for corneal-based procedures, particularly when presbyopia significantly affects daily function.
Conductive Keratoplasty
Conductive keratoplasty uses radiofrequency energy delivered via a fine probe to specific points in the peripheral cornea, causing collagen fibers to shrink and steepen the central cornea. This non-laser approach treats low hyperopia and presbyopia. According to EyeWiki, CK achieved uncorrected visual acuity of 20/40 or better in more than 89% of eyes for correction of hyperopia and astigmatism. However, CK has largely fallen out of favor due to high rates of regression, where the initial corrective effect diminishes over several years. While the procedure demonstrated promising short-term results, its lack of long-term durability limits its role in modern refractive practice.
With these procedure types defined, the next step is understanding how each one works in greater detail.
How Does LASIK Work Step by Step?
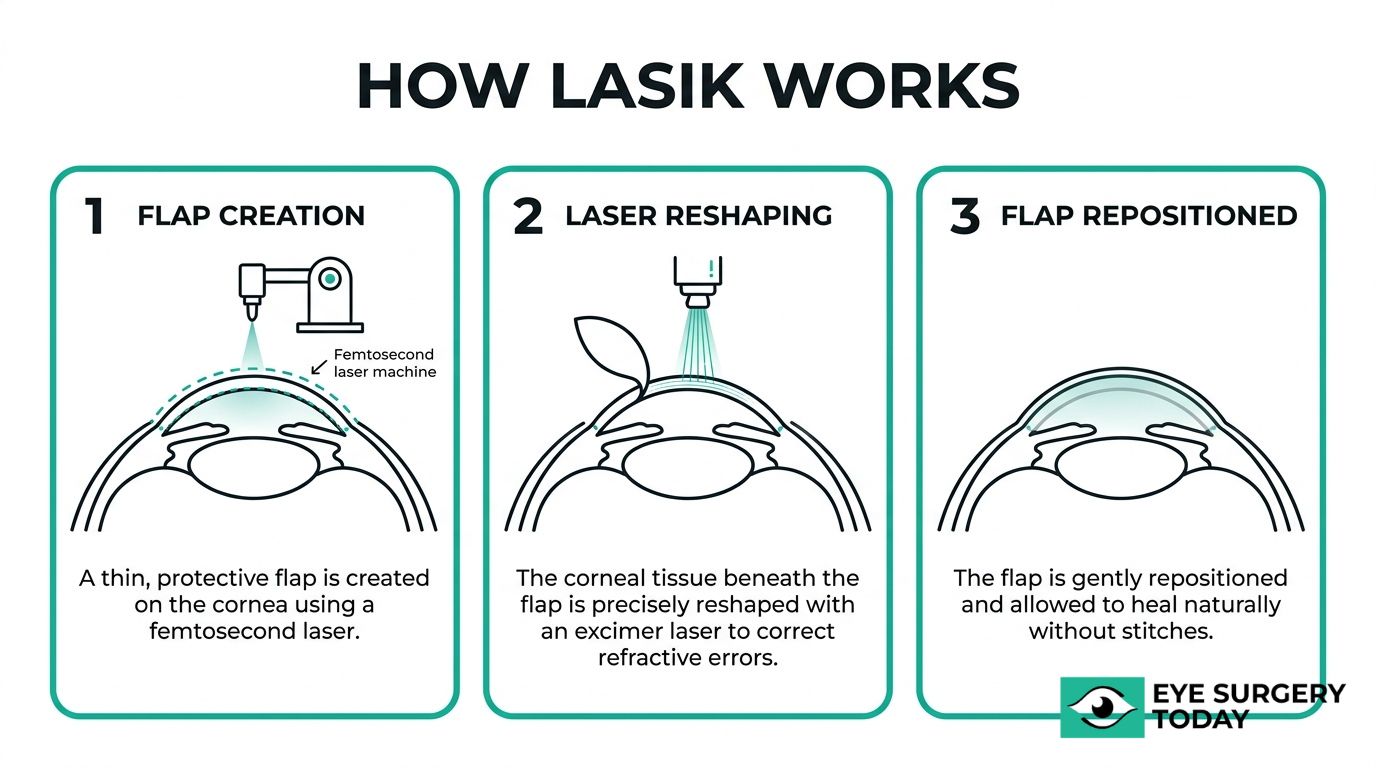
LASIK works by reshaping the cornea with two precise lasers to correct how light focuses on the retina. The procedure follows three key stages: flap creation, stromal reshaping, and flap repositioning.
First, the surgeon applies numbing eye drops and places a small device to hold the eyelid open. A femtosecond laser then creates a thin, hinged corneal flap on the surface of the eye. This flap, typically around 100 to 120 microns thick, is gently lifted to expose the underlying stromal tissue.
Next, an excimer laser removes microscopic amounts of corneal tissue based on a pre-programmed treatment map. For myopia, the laser flattens the central cornea. For hyperopia, it steepens the central area. For astigmatism, it smooths irregularities into a more uniform shape. The entire reshaping process usually takes less than a minute per eye.
Finally, the surgeon repositions the corneal flap over the treated area. According to the U.S. Food and Drug Administration, the flap adheres naturally without stitches, and initial healing begins within hours. Because the flap preserves the outer epithelial layer, recovery tends to be faster than surface-based procedures.
The precision of this two-laser approach, combining the femtosecond laser for flap creation with the excimer laser for tissue reshaping, is what gives LASIK its rapid visual recovery and high patient satisfaction. Understanding this process can help clarify how LASIK differs from other refractive procedures.
How Does LASIK Compare to Other Refractive Procedures?
LASIK compares favorably to other refractive procedures in speed of recovery and visual outcomes, though each alternative offers distinct advantages for specific patient profiles. The following sections break down how LASIK differs from PRK, SMILE, ICL, and refractive lens exchange.
How Does LASIK Compare to PRK?
LASIK compares to PRK primarily in surgical technique and recovery timeline. LASIK creates a corneal flap to access the underlying stroma, while PRK removes the outer epithelial layer entirely before reshaping the cornea with an excimer laser. Both procedures use the same excimer laser technology to correct refractive errors, so final visual outcomes can be very similar.
The most significant difference is recovery. LASIK patients typically notice improved vision within hours, whereas PRK requires days of epithelial regrowth before vision begins to clear. PRK may be the better option for patients with thinner or more irregular corneas where creating a flap could be risky. Because PRK involves no flap, it also eliminates flap-related complications entirely.
For patients who meet LASIK candidacy requirements, the faster recovery often makes it the preferred choice. However, when corneal anatomy limits flap creation, PRK can deliver comparable long-term results.
How Does LASIK Compare to SMILE?
LASIK compares to SMILE in the way each procedure accesses and reshapes corneal tissue. LASIK requires a corneal flap created by a femtosecond laser, followed by excimer laser reshaping. SMILE is a flapless procedure; a femtosecond laser creates a small lenticule within the intact cornea, which the surgeon removes through a tiny incision.
According to a 2025 comparison published in The Ophthalmologist, both procedures deliver similar visual acuity outcomes for myopia correction. The flapless design of SMILE may preserve more corneal nerve fibers, which can reduce post-operative dry eye symptoms in some patients. SMILE also involves a smaller incision, potentially offering greater biomechanical stability.
LASIK, however, treats a broader range of refractive errors, including hyperopia and higher levels of astigmatism. SMILE is currently approved primarily for myopia and myopic astigmatism. For patients whose prescription falls within SMILE’s treatment range, the choice often comes down to surgeon recommendation and individual corneal characteristics.
How Does LASIK Compare to ICL?
LASIK compares to ICL in treatment location and reversibility. LASIK permanently reshapes the cornea using an excimer laser, while ICL involves implanting a phakic intraocular lens behind the iris and in front of the natural lens. This distinction makes ICL a reversible procedure, since the lens can be removed or exchanged if needed.
ICL is often recommended for patients with moderate to high myopia, thin corneas, or severe dry eyes who may not qualify for corneal laser procedures. Because ICL does not remove corneal tissue, it preserves the cornea’s original structure entirely. Recovery after ICL is typically rapid, with noticeable improvement within a day or two.
LASIK remains the more commonly performed procedure for mild to moderate refractive errors due to its shorter procedure time, lower cost, and well-established long-term track record. For patients with higher prescriptions or corneal limitations, ICL can achieve excellent visual correction where LASIK may not be suitable.
How Does LASIK Compare to Refractive Lens Exchange?
LASIK compares to refractive lens exchange in target anatomy and ideal patient age. LASIK reshapes the cornea, while RLE replaces the eye’s natural crystalline lens with an artificial intraocular lens. RLE is typically reserved for patients over 40 with high hyperopia or presbyopia who are not ideal LASIK candidates.
Dr. Robert Maloney, M.D. of the Maloney-Shamie Vision Institute, describes LASIK as “sculpting a contact lens onto the surface of your eye” to provide vision often better than a contact lens without the inconvenience of wearing one. This corneal approach works well for younger patients with stable prescriptions. RLE, by contrast, addresses vision correction at the lens level and simultaneously eliminates the possibility of future cataract development, since the natural lens has already been replaced.
LASIK offers faster recovery and lower surgical risk for eligible candidates. RLE carries a higher risk profile and greater cost, but it may be the only viable path to spectacle independence for patients whose age or refractive error places them outside LASIK’s treatment range.
With these procedural differences in mind, the next step is understanding who qualifies as a good candidate for each option.
Who Is a Good Candidate for Refractive Vision Correction?
A good candidate for refractive vision correction depends on factors like age, prescription strength, corneal thickness, and overall eye health. The best procedure varies by individual profile.
Who Is an Ideal Candidate for LASIK?
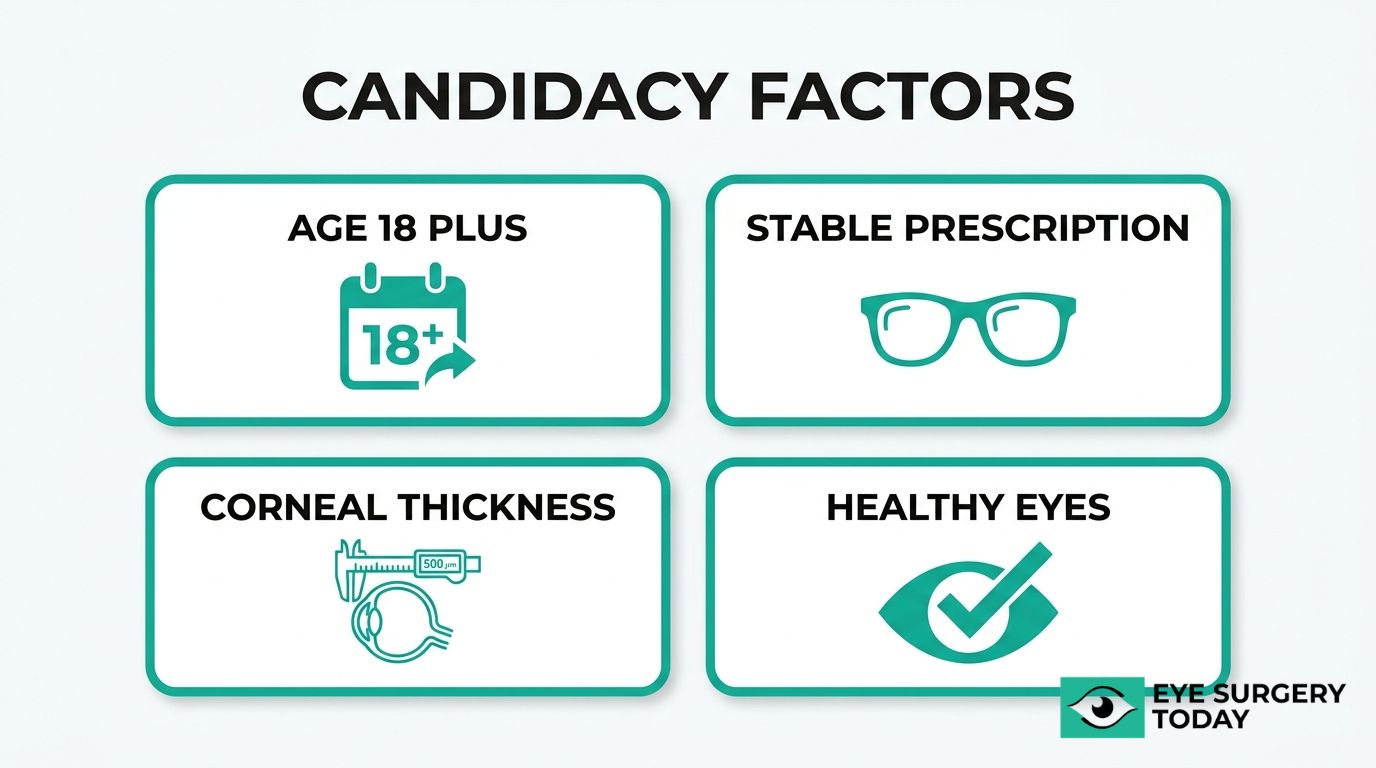
An ideal candidate for LASIK is at least 18 years old with a stable prescription, adequate corneal thickness, and no active eye disease. According to clinical guidelines published in CRSToday, current FDA approvals for LASIK generally allow treatment of myopia up to -12.00 D, astigmatism up to 6.00 D, and hyperopia up to 6.00 D, depending on the specific laser platform used.
Candidates should be free of conditions such as:
- Keratoconus or corneal ectasia
- Severe dry eye syndrome
- Uncontrolled glaucoma
- Autoimmune disorders that impair healing
Pregnancy and nursing can temporarily shift refraction, so most surgeons advise waiting until hormonal stability returns. In practice, the corneal evaluation is the single most important screening step; even patients with otherwise perfect candidacy profiles may be redirected to an alternative procedure if corneal mapping reveals irregularities.
Who May Be a Better Candidate for PRK Instead of LASIK?
A better candidate for PRK instead of LASIK is someone with thinner or more irregular corneas where creating a LASIK flap may be contraindicated. Because PRK reshapes the corneal surface without cutting a flap, it preserves more stromal tissue and reduces the risk of flap-related complications.
PRK may also be preferred for patients who:
- Have occupations or hobbies with high impact risk, such as military service or contact sports
- Present with mild corneal surface irregularities detected during topography
- Have borderline corneal thickness that falls below safe LASIK thresholds
Although PRK delivers visual outcomes comparable to LASIK over time, the longer initial recovery period is worth weighing. For patients whose corneal anatomy rules out a flap, PRK remains one of the most reliable surface ablation options available.
Who Should Consider ICL Over Laser-Based Procedures?
Patients who should consider ICL over laser-based procedures are those with high refractive errors, thin corneas, or severe dry eyes that make corneal reshaping unsuitable. ICL surgery involves implanting a phakic intraocular lens behind the iris and in front of the natural lens, correcting moderate to high myopia and astigmatism without removing corneal tissue.
ICL candidates typically share these characteristics:
- Myopia beyond the treatable range for LASIK or PRK
- Insufficient corneal thickness for safe laser ablation
- Chronic dry eye that corneal surgery could worsen
- Age between 21 and 45 with a stable prescription
Because ICL is additive rather than subtractive, it preserves the cornea’s structural integrity entirely. This reversibility makes it a particularly appealing choice for younger patients with extreme prescriptions who want to keep future surgical options open.
Who Might Benefit More from Refractive Lens Exchange?
Patients who might benefit more from refractive lens exchange are typically adults over 40 with high hyperopia, presbyopia, or early lens changes that make corneal procedures less effective. RLE replaces the eye’s natural lens with an artificial intraocular lens, correcting the refractive error at its source while also eliminating the future need for cataract surgery.
RLE may be well suited for individuals who:
- Have high farsightedness beyond laser correction thresholds
- Experience progressive presbyopia limiting near and intermediate vision
- Show early cataract formation that would eventually require lens replacement
- Seek premium IOL options, such as multifocal or trifocal lenses, for broader spectacle independence
According to the American Academy of Ophthalmology, risks of RLE include retinal detachment, particularly in high myopes, with reported incidences ranging from 1% to 3%. This risk profile means thorough retinal evaluation before surgery is essential. RLE costs in the U.S. typically range from $2,500 to $8,000 per eye, with premium IOL selection driving the higher end.
Understanding your candidacy profile is the first step; knowing what to expect from potential benefits and risks helps refine that decision further.
What Are the Potential Benefits of Refractive Vision Correction?
The potential benefits of refractive vision correction include improved visual acuity, reduced dependence on glasses or contact lenses, and enhanced quality of life.
- Improved visual clarity. Clinical studies indicate that between 96% and 99% of patients achieve 20/20 vision or better following a single laser vision correction procedure, according to the Refractive Surgery Council. This level of precision can transform daily activities, from driving to reading, without corrective lenses.
- Reduced dependence on glasses and contacts. Modern refractive procedures offer high rates of spectacle independence. For LASIK, many patients achieve freedom from glasses and contact lenses for most routine activities.
- Enhanced quality of life. A 2025 assessment published on the National Institutes of Health reported that 82% of refractive surgery patients expressed high levels of satisfaction and 93% noted an improved quality of life following their procedure.
- Greater convenience for active lifestyles. Without the need for daily lens care, cleaning solutions, or backup glasses, patients often find sports, travel, and outdoor activities significantly easier to manage.
- Long-term financial value. Although refractive procedures require an upfront investment, the cumulative cost of glasses, contact lenses, and lens care products over decades can exceed the one-time cost of surgery for many individuals.
For most patients with stable refractive errors, the combination of high visual outcomes and lasting satisfaction makes refractive vision correction one of the most impactful elective procedures available today. Understanding these benefits is important, but so is weighing them against the possible risks and side effects covered next.
What Are the Possible Risks and Side Effects of Refractive Surgery?
The possible risks and side effects of refractive surgery vary by procedure type. The sections below cover specific risks associated with LASIK, PRK, SMILE, and ICL.
What Are the Possible Risks of LASIK?
The possible risks of LASIK include dry eye symptoms, visual disturbances, and rare but serious complications such as infection or flap dislocation. According to the American Refractive Surgery Council, serious sight-threatening complications from LASIK occur in less than 1% of cases, including infections and dislocation of the corneal flap.
Temporary side effects are more common. Up to 30% of patients may experience dry eye symptoms within the first three months after surgery, though most cases improve as the eye heals over 6 to 12 months. Glare, halos, and starbursts around lights at night can also occur during the stabilization period. Because LASIK involves creating a corneal flap, flap-related issues, while uncommon, represent a unique risk not shared by flapless procedures. For most patients, the overall complication profile remains low when proper candidacy screening is followed.
What Are the Possible Risks of PRK?
The possible risks of PRK include prolonged discomfort during the healing period, corneal haze, and a slower visual recovery compared to LASIK. Because PRK removes the outer corneal epithelium rather than creating a flap, there is no risk of flap complications. However, the exposed corneal surface requires more time to regenerate, which can increase the chance of infection during the early postoperative days.
Corneal haze may develop in some patients as the epithelium heals, particularly with higher corrections. Dry eye and temporary visual disturbances, such as glare or halos, can also occur. These side effects tend to resolve gradually as the cornea stabilizes, though full recovery may take longer than with LASIK. Mitomycin C, an anti-scarring agent, is often applied during surgery to reduce the risk of haze. Despite the extended healing timeline, PRK remains a well-established procedure with a favorable long-term safety profile.
What Are the Possible Risks of SMILE?
The possible risks of SMILE include dry eye, visual disturbances, and difficulty with the lenticule extraction step. As a flapless procedure, SMILE eliminates the risk of flap dislocation entirely. However, the small incision used to remove the lenticule may occasionally present surgical challenges, particularly in complex cases.
Temporary dry eye can occur after SMILE, though some evidence suggests it may be less frequent than with LASIK because fewer corneal nerves are disrupted. Halos and glare around lights at night are possible during recovery, especially in the early weeks. In rare cases, small lenticule remnants or an incomplete extraction may require additional intervention. Overall, the risk profile of SMILE is considered comparable to other laser-based refractive procedures, and most side effects tend to be temporary.
What Are the Possible Risks of ICL?
The possible risks of ICL include elevated intraocular pressure, cataract formation, and endothelial cell loss over time. Because ICL surgery involves placing a phakic intraocular lens inside the eye, behind the iris and in front of the natural lens, it carries risks distinct from corneal-based procedures.
Elevated intraocular pressure can occur shortly after implantation and typically requires monitoring in the early postoperative period. If the ICL is improperly sized, it may vault too close to the natural lens, potentially accelerating cataract development. Endothelial cell loss, while generally gradual, is another consideration for long-term follow-up. Infection, though rare, poses a risk with any intraocular procedure. One advantage of ICL is its reversibility; the lens can be removed or exchanged if complications arise. Patients considering ICL should discuss these risks thoroughly with their surgeon to determine whether the benefits outweigh the potential concerns.
Understanding each procedure’s risk profile is an important step before exploring what recovery looks like.
What Should You Expect During Recovery from Refractive Surgery?
Recovery from refractive surgery varies by procedure, with each method following a distinct healing timeline. The sections below cover what to expect after LASIK, PRK, SMILE, and ICL. Other eye procedures, such as eyelid surgery, involve their own specific recovery considerations, highlighting the diversity of post-operative care across ophthalmic treatments.
What Is Recovery Like After LASIK?
Recovery after LASIK is generally rapid, with most patients noticing improved vision within hours of the procedure. However, the initial clarity can be misleading; full visual stabilization typically takes longer than many people expect.
According to the U.S. Food and Drug Administration (FDA), visual stabilization after LASIK typically takes three to six months, during which patients may experience fluctuating vision, glare, and halos. Common early symptoms include:
- Mild burning or itching for a few hours after surgery
- Light sensitivity and watery eyes during the first day
- Temporary dry eye that may persist for weeks
- Halos or glare around lights, particularly at night
Most patients can return to normal activities within a day or two, though eye rubbing must be avoided to protect the corneal flap. Follow-up appointments in the days and weeks after surgery allow the surgeon to monitor healing progress. For anyone accustomed to quick fixes, patience during the stabilization window is essential; the best visual outcomes often emerge gradually.
What Is Recovery Like After PRK?
Recovery after PRK is slower than LASIK because the procedure removes the outer corneal layer, called the epithelium, which must regenerate naturally. Initial vision blurring is common, with gradual improvement over three to five days as the epithelium heals. Full visual recovery and stabilization can take a month or longer, according to the American Academy of Ophthalmology.
During the first few days, patients typically wear a protective bandage contact lens to reduce discomfort while the surface heals. Pain and light sensitivity tend to be more noticeable than with LASIK, and prescription eye drops help manage inflammation and prevent infection. Because the recovery window is extended, PRK requires more patience; however, the absence of a corneal flap eliminates flap-related complications entirely. Most daily activities can resume within a week, though strenuous exercise and swimming should be avoided for several weeks.
What Is Recovery Like After SMILE?
Recovery after SMILE falls between LASIK and PRK in terms of speed. Because SMILE uses a small incision rather than a corneal flap, the structural integrity of the cornea remains largely intact, which can contribute to a comfortable healing process. Most patients notice meaningful visual improvement within the first two to three days, though mild blurriness and light sensitivity may linger for a week or so.
Discomfort after SMILE tends to be minimal, often described as slight grittiness or dryness. Lubricating eye drops are typically recommended during the first few weeks. Since no flap is created, there is no risk of flap displacement during recovery, which makes post-operative restrictions somewhat less demanding. Patients can usually return to desk work and light activities within a day or two. Full visual sharpness may take a few weeks to stabilize as the cornea settles into its new shape.
What Is Recovery Like After ICL?
Recovery after ICL surgery is typically rapid, with significant visual improvement often noted within a day or two and full stabilization within a few weeks, according to the American Academy of Ophthalmology. Because the procedure involves placing a lens inside the eye rather than reshaping the cornea, surface healing is minimal.
Patients can expect:
- Noticeable vision improvement within 24 to 48 hours
- Mild soreness or light sensitivity for the first day
- Use of anti-inflammatory and antibiotic eye drops for several weeks
- Routine follow-up visits to check lens position and intraocular pressure
Most people resume normal activities within a few days, though heavy lifting and swimming should be avoided in the short term. The rapid recovery timeline makes ICL particularly appealing for patients with high prescriptions who need quick visual rehabilitation. Of all the procedures covered here, ICL generally offers the fastest return to functional vision.
Understanding each procedure’s recovery timeline helps set realistic expectations before surgery day.
How Much Does Refractive Vision Correction Cost?
Refractive vision correction costs vary by procedure type, technology used, and surgeon experience. The sections below cover typical price ranges for LASIK, PRK, SMILE, and ICL.
How Much Does LASIK Typically Cost?
LASIK typically costs between $1,500 and $3,500 per eye in the United States. According to NVISION Eye Centers, the average cost of LASIK surgery in 2025 is approximately $2,632 per eye, with pricing influenced by the laser platform, surgeon experience, and geographic location.
Several factors can shift the final price:
- Wavefront-guided or custom LASIK treatments often cost more than standard procedures.
- All-laser (bladeless) LASIK using a femtosecond laser to create the corneal flap tends to be priced higher than microkeratome-assisted options.
- Comprehensive packages that include pre-operative evaluations, post-operative care visits, and enhancement policies may carry a premium but reduce unexpected out-of-pocket expenses.
Most vision insurance plans classify LASIK as an elective procedure and do not cover it. However, many practices offer financing plans, and patients can often use health savings accounts (HSAs) or flexible spending accounts (FSAs) to offset costs.
How Much Does PRK Typically Cost?
PRK typically costs between $1,500 and $3,000 per eye, making it comparable to or slightly less expensive than LASIK. Because PRK does not require creating a corneal flap, the procedure uses fewer surgical instruments, which can contribute to marginally lower fees at some practices.
Pricing still depends on several variables:
- The excimer laser platform and any wavefront-guided customization applied during treatment.
- Whether the quoted fee includes bandage contact lenses, prescription eye drops, and follow-up appointments during the longer healing period.
- Geographic market and the surgeon’s level of specialization.
PRK is generally considered elective, so insurance coverage is uncommon. For patients with thinner corneas who cannot qualify for LASIK, PRK represents a cost-effective alternative that delivers comparable long-term visual outcomes. Asking your surgeon’s office for a detailed breakdown of what the quoted fee includes helps avoid surprise charges during recovery.
How Much Does SMILE Typically Cost?
SMILE typically costs between $2,000 and $4,000 per eye. This places it at the higher end of laser-based refractive procedures, largely because the femtosecond laser technology required for lenticule extraction involves specialized equipment and training.
Factors that influence SMILE pricing include:
- The specific femtosecond laser platform (currently limited to fewer manufacturers than LASIK platforms).
- Surgeon expertise with the flapless extraction technique.
- Whether the practice bundles post-operative care, enhancement guarantees, and follow-up visits into one fee.
Because SMILE is a newer procedure with fewer competing platforms, pricing tends to be less variable across practices than LASIK. Patients should confirm whether their quoted fee covers all follow-up appointments and any potential retreatment. Like other refractive procedures, SMILE is typically classified as elective and not covered by standard vision insurance.
How Much Does ICL Typically Cost?
ICL typically costs between $3,000 and $5,000 per eye, making it one of the more expensive refractive correction options. According to Berkeley Eye Center, costs can increase further depending on the specific Implantable Collamer Lens type, whether toric correction for astigmatism is included, and the surgeon’s expertise.
The higher price reflects several factors:
- ICL involves implanting a phakic intraocular lens inside the eye, requiring microsurgical skills and an operating room setting.
- Pre-operative testing is more extensive, often including anterior chamber depth measurements and endothelial cell counts.
- The lens itself is a custom-manufactured medical device, adding material costs that laser procedures do not carry.
For patients with high myopia or thin corneas who are not candidates for LASIK or SMILE, ICL may represent the only viable surgical option. HSA and FSA funds can typically be applied toward ICL costs, and many practices offer payment plans.
Understanding procedure-specific pricing helps narrow down which options fit both your visual needs and your budget.
How Long Do the Results of Refractive Surgery Last?
The results of refractive surgery can last many years, though long-term stability varies by procedure type and individual factors. LASIK and PRK reshape the cornea permanently, so the structural correction itself does not reverse. However, the eye can still change over time due to natural aging, progressive myopia, or the eventual onset of presbyopia after age 40. These changes may gradually reduce the clarity achieved immediately after surgery, leading some patients to need glasses for certain tasks or consider an enhancement procedure later.
According to a 15-year follow-up study published in ScienceDirect on ICL implantation for high myopia, the procedure demonstrated long-term stability and effectiveness, though common complications included vision changes and intraocular pressure shifts. Lens-based procedures like refractive lens exchange offer a different durability profile: because the natural lens is replaced entirely, the corrective power of the artificial intraocular lens remains stable indefinitely and eliminates future cataract development in that eye.
Not all procedures hold their correction equally well. Conductive keratoplasty, for instance, has largely fallen out of favor due to high rates of regression over several years, where the initial corrective effect gradually diminishes. For patients considering any refractive procedure, discussing expected longevity with a surgeon helps set realistic expectations about whether enhancements or reading glasses may eventually become necessary.
What Questions Should You Ask Your Surgeon Before Refractive Surgery?
The questions you should ask your surgeon before refractive surgery cover candidacy, procedure specifics, expected outcomes, risks, costs, and recovery. Preparing these questions in advance helps ensure a thorough consultation and a confident decision.
- Am I a good candidate for this procedure? Ask whether your corneal thickness, prescription stability, and overall eye health qualify you for the recommended procedure, or if an alternative such as PRK, SMILE, or ICL may be more appropriate.
- What specific results can I realistically expect? Request clarity on the likelihood of achieving your target vision, whether you may still need glasses for certain tasks, and how your prescription range affects predicted outcomes.
- What are the risks and possible side effects? Ask about both common side effects, such as dry eye and visual disturbances, and rare but serious complications specific to the procedure being recommended.
- What does the total cost include? Confirm whether the quoted price covers pre-operative evaluations, the surgery itself, post-operative visits, and any enhancement procedures if results need refinement.
- What is the recovery timeline? Ask how soon you can return to work, drive, and resume physical activities, and when your vision is expected to fully stabilize.
- How many of these procedures have you performed? Surgeon experience directly influences outcomes, so asking about volume and complication rates is reasonable and important.
- What technology do you use? Inquire whether the practice uses wavefront-guided treatment, femtosecond laser flap creation, or other advanced platforms that may affect precision and safety.
- What happens if my vision changes years later? Ask whether enhancement procedures are available, whether they are included in your surgical fee, and what long-term follow-up looks like.
According to a 2025 assessment published in the National Institutes of Health, 82% of refractive surgery patients expressed high satisfaction and 93% noted improved quality of life following their procedure. These strong outcomes reinforce the value of a well-prepared consultation. Patients who walk into their appointment with specific, targeted questions tend to leave with greater confidence in their surgical plan, and that confidence often translates into a smoother overall experience.
How Can Surgeon-Reviewed Education Help You Choose the Right Refractive Procedure?
Surgeon-reviewed education can help you choose the right refractive procedure by providing unbiased, clinically accurate information about every major option. The sections below cover how Eye Surgery Today supports that decision and the key takeaways from this guide.
Can Eye Surgery Today Help You Understand Your Refractive Surgery Options?
Yes, Eye Surgery Today can help you understand your refractive surgery options. The platform provides surgeon-reviewed educational content covering LASIK, PRK, SMILE, ICL, and refractive lens exchange, with clear candidacy thresholds and head-to-head comparisons that many other resources lack.
Each guide explains the technologies involved in modern vision correction, from excimer and femtosecond lasers to phakic IOLs and wavefront-guided platforms. Eye Surgery Today breaks down what these terms mean in plain language so readers can evaluate their options with confidence.
According to a 2025 assessment published in the National Institutes of Health (PMC), 82% of refractive surgery patients expressed high satisfaction and 93% reported improved quality of life following their procedure. Understanding procedural differences, realistic recovery timelines, and potential side effects before surgery may contribute to outcomes like these. Eye Surgery Today organizes this information in one accessible, surgeon-reviewed resource designed to empower patients rather than overwhelm them.
What Are the Key Takeaways About Refractive Vision Correction We Covered?
The key takeaways about refractive vision correction covered in this guide are:
- Refractive errors, including myopia, hyperopia, astigmatism, and presbyopia, affect billions of people worldwide and can be addressed through several proven surgical approaches.
- LASIK, PRK, SMILE, ICL, and refractive lens exchange each serve different visual profiles, corneal characteristics, and lifestyle needs.
- According to the Refractive Surgery Council, between 96% and 99% of patients achieve 20/20 vision or better after a single laser vision correction procedure.
- Candidacy depends on factors such as age, prescription stability, corneal thickness, and the presence of conditions like dry eye or keratoconus.
- Cost, recovery timeline, and risk profile vary significantly across procedures, making a thorough comparison essential before committing.
- Surgeon-reviewed resources can help bridge the gap between complex clinical information and practical patient understanding.
The most important step in choosing refractive vision correction is a comprehensive eye examination with a qualified surgeon who can match the right procedure to your specific anatomy and visual goals.





