Cataract surgery is a procedure that removes the eye’s clouded natural lens and replaces it with a clear artificial intraocular lens (IOL). It is one of the most commonly performed surgical procedures in the United States, and no medication or eye drop can reverse the protein aggregation that causes lens clouding.
This guide covers candidacy and coexisting conditions, surgical techniques and lens options, pre-operative preparation and the procedure itself, recovery timelines and activity restrictions, and potential risks, costs, and long-term results.
Candidacy for cataract surgery depends on how significantly cataracts affect daily functioning, and patients with conditions such as glaucoma, diabetes, macular degeneration, or prior LASIK may still qualify with specialized planning and realistic expectations set beforehand.
Three primary surgical techniques are available, including standard phacoemulsification, extracapsular extraction for very advanced cataracts, and femtosecond laser-assisted surgery. IOL selection ranges from standard monofocal lenses to premium multifocal, extended depth of focus, toric, and light adjustable designs, each targeting different visual needs.
Preparation involves a detailed pre-operative eye exam with precise biometry measurements, medication adjustments, and logistics planning for surgery day. The procedure itself typically takes 10 to 30 minutes under topical anesthesia.
Full recovery generally spans four to eight weeks, with most patients noticing clearer vision within days. Specific timelines guide when driving, exercise, showering, and travel may safely resume.
While serious complications are uncommon, conditions such as posterior capsule opacification, infection, and cystoid macular edema are possible; recognizing warning signs early supports the best outcomes. Cost varies based on insurance coverage and lens choice, with standard lenses typically covered and premium upgrades requiring additional out-of-pocket expense.
What Is Cataract Surgery?
Cataract surgery is a procedure that removes the eye’s clouded natural lens and replaces it with a clear artificial intraocular lens (IOL). More than 3.5 million cataract operations are performed annually in the United States, according to a 2025 report published in JAMA, making it one of the most common surgical procedures in high-income countries. The clouding typically develops gradually as proteins in the lens break down with age, progressively blurring vision and reducing contrast sensitivity. Because no medication or eye drop can reverse this protein aggregation, surgical removal remains the only definitive treatment. During the procedure, the surgeon creates a small incision, breaks apart and removes the opaque lens material, and inserts a replacement IOL tailored to the patient’s visual needs. Most patients undergo the operation on an outpatient basis under local or topical anesthesia, returning home the same day. For patients navigating this decision, understanding the basics of how the procedure works can make the entire experience, from pre-operative planning through recovery, feel far more manageable.
Who May Be a Good Candidate for Cataract Surgery?
A good candidate for cataract surgery is typically someone whose cataracts interfere with daily activities and quality of life. Candidacy depends on cataract severity, coexisting eye conditions, and overall ocular health.

How Do You Know When Cataracts Are Bad Enough for Surgery?
You know when cataracts are bad enough for surgery when vision loss begins interfering with everyday tasks, such as driving, reading, or recognizing faces. A cataract diagnosis alone does not automatically mean surgery is needed. The decision typically depends on how significantly the clouding affects functional vision, not just what an eye exam reveals.
Common indicators that may suggest it is time to consider surgery include:
- Difficulty driving at night due to glare or halos around lights.
- Frequent prescription changes that no longer improve vision adequately.
- Trouble reading or seeing fine details even with corrective lenses.
- Colors appearing faded, washed out, or yellowed.
- Increasing difficulty performing work-related or recreational activities.
Your ophthalmologist may recommend surgery when corrective lenses can no longer compensate for the vision loss caused by the cataract. In many cases, patients wait too long because vision decline happens gradually, making it harder to recognize how much functional ability has been lost.
Can You Get Cataract Surgery if You Have Glaucoma?
Yes, you can get cataract surgery if you have glaucoma, though the procedure requires additional planning. Glaucoma does not automatically disqualify someone from cataract surgery; in fact, some patients experience a modest reduction in intraocular pressure after lens replacement.
However, careful coordination between cataract and glaucoma management is essential. According to the American Academy of Ophthalmology, proper planning and management of the ocular surface are critical for patients with comorbid glaucoma, as ocular surface disease is common in this population and can affect surgical outcomes. Surgeons may also evaluate whether a combined procedure, sometimes called minimally invasive glaucoma surgery performed alongside cataract removal, is appropriate.
Patients with advanced glaucoma should discuss realistic visual expectations with their surgeon, since pre-existing optic nerve damage may limit the degree of vision improvement achievable through cataract surgery alone.
Can You Get Cataract Surgery if You Have Macular Degeneration?
Yes, you can get cataract surgery if you have macular degeneration, but visual outcomes may be more limited compared to patients without retinal disease. Cataract removal can improve overall clarity and light transmission through the eye, which often helps peripheral and functional vision even when central vision is compromised by macular degeneration.
The key consideration involves setting realistic expectations. Because macular degeneration affects the macula, the area responsible for sharp central vision, removing the cataract may not fully restore reading ability or fine detail recognition. Still, reducing the cloudiness caused by a cataract can improve contrast sensitivity and make daily activities easier.
Ophthalmologists typically assess the severity of macular degeneration before recommending surgery. In practice, patients with stable, dry macular degeneration tend to benefit more predictably than those with active wet macular degeneration, where ongoing retinal changes may complicate the recovery timeline.
Can You Get Cataract Surgery if You Have Diabetes?
Yes, you can get cataract surgery if you have diabetes, provided blood sugar levels are reasonably well controlled and any diabetic eye disease is properly managed beforehand. Diabetes does not disqualify someone from the procedure, though it does introduce considerations that require closer monitoring.
Diabetic patients face a higher risk of developing postoperative complications, such as diabetic macular edema or delayed healing. Surgeons typically evaluate the retina carefully before proceeding, and any active diabetic retinopathy may need treatment prior to cataract removal.
Key factors that influence candidacy for diabetic patients include:
- Current hemoglobin A1c levels and blood sugar stability.
- Presence or absence of diabetic retinopathy or macular edema.
- Overall health of the retinal blood vessels.
- Ability to follow postoperative medication and follow-up schedules.
Well-managed diabetic patients often achieve excellent outcomes from cataract surgery, making preoperative optimization of blood sugar and retinal health one of the most important steps in the process.
Can You Get Cataract Surgery if You Have Had LASIK?
Yes, you can get cataract surgery if you have had LASIK. According to a 2025 report in Frontiers in Medicine, post-LASIK patients are candidates for cataract surgery, but they require specialized IOL power calculations due to previous corneal alterations, and surface abnormalities may limit candidacy for certain elective multifocal IOLs.
The primary challenge involves accurately measuring the eye for the replacement lens. LASIK reshapes the cornea, which changes the standard measurements surgeons rely on to calculate IOL power. Without specialized formulas, there is a greater risk of a refractive surprise, meaning the final prescription may not match the intended target.
Modern biometry tools and post-refractive IOL calculation methods have significantly improved accuracy for these patients. Sharing prior LASIK records, including pre-LASIK corneal measurements, with the cataract surgeon helps ensure the most precise lens selection possible.
With the right candidacy factors addressed, understanding the types of cataract surgery available becomes the next step in preparing for the procedure.
What Are the Types of Cataract Surgery?
The types of cataract surgery are phacoemulsification, extracapsular cataract extraction, and femtosecond laser-assisted cataract surgery. Each technique differs in incision size, technology used, and suitability for specific cataract severities.
Phacoemulsification
Phacoemulsification is the most widely performed type of cataract surgery. This technique uses ultrasonic energy to break the cloudy lens into small fragments, which are then suctioned out through a small incision, typically 2 to 3 mm in length. An artificial intraocular lens is inserted through the same micro-incision to replace the natural lens.
Because the incision is small, phacoemulsification generally requires no sutures and promotes faster healing. Most surgeons consider it the standard of care for the majority of cataract cases due to its predictable outcomes and minimal tissue disruption. However, extremely dense or advanced cataracts may require an alternative approach when ultrasonic fragmentation alone cannot safely break down the lens material.
Extracapsular Cataract Extraction
Extracapsular cataract extraction (ECCE) is a surgical technique that removes the lens nucleus in one piece through a larger incision. According to the American Academy of Ophthalmology, ECCE typically requires an incision of 10 to 12 mm and is generally reserved for very advanced cataracts where phacoemulsification may not be safe.
The larger incision usually requires sutures, which can extend recovery time compared to phacoemulsification. Despite this, ECCE remains a valuable option when the cataract has hardened beyond what ultrasonic energy can efficiently fragment. For patients with very mature or white cataracts, this approach may offer a safer pathway to lens removal.
Femtosecond Laser-Assisted Cataract Surgery
Femtosecond laser-assisted cataract surgery (FLACS) uses ultrashort laser pulses to perform the anterior capsulotomy and lens fragmentation steps that are done manually during conventional phacoemulsification. This added precision can create more consistent capsular openings and soften the lens before ultrasonic removal.
A meta-analysis of 46 randomized controlled trials involving 8,871 eyes, published in Scientific Reports, found that FLACS yielded significantly better corrected distance visual acuity one week postoperatively (P = 0.011), but no significant differences were observed beyond one week or in overall complications (P = 0.999). For most patients, conventional phacoemulsification remains highly effective, though FLACS may appeal to those seeking the precision of laser guidance during specific surgical steps.
With the surgical approach selected, the next consideration is choosing the right intraocular lens.
What Types of Intraocular Lenses Can Be Used?
The types of intraocular lenses that can be used during cataract surgery include monofocal, multifocal, extended depth of focus, toric, and light adjustable designs. Each IOL type targets different vision needs. Understanding lifestyle factors and personal vision goals is key when choosing the right IOL for optimal post-surgical vision.

Monofocal IOL
A monofocal IOL is an intraocular lens that corrects vision at one fixed focal point, typically set for distance. Patients who choose a monofocal lens can usually see clearly at far range but will likely need reading glasses for near tasks. According to a 2025 systematic review published in Eye (Nature), enhanced monofocal intraocular lenses, such as the Eyhance IOL, offer a clinically relevant improvement in intermediate and near vision compared to standard monofocal IOLs. This makes enhanced monofocal designs a practical middle ground for patients who want some functional range without the visual trade-offs that come with multifocal optics.
Multifocal IOL
A multifocal IOL is a premium intraocular lens designed to provide clear vision at multiple distances, including near, intermediate, and far. The lens uses concentric rings or zones to split incoming light into separate focal points. While this design can significantly reduce dependence on glasses after cataract surgery, some patients may notice visual phenomena such as halos or glare, particularly at night. Multifocal IOLs tend to work best for patients with healthy retinas and minimal astigmatism who prioritize spectacle independence.
Extended Depth of Focus IOL
An extended depth of focus (EDOF) IOL is an intraocular lens that elongates a single focal point rather than splitting light into multiple zones. This design provides a continuous range of vision from distance through intermediate, with fewer halos and glare compared to multifocal lenses. Near vision, however, may still require reading glasses in low-light conditions or for very fine print. For patients who spend significant time on computers or driving, EDOF lenses often represent a strong balance between visual range and optical quality.
Toric IOL
A toric IOL is an intraocular lens specifically engineered to correct pre-existing corneal astigmatism during cataract surgery. The lens has different optical powers along its meridians, which compensate for the uneven curvature of an astigmatic cornea. Precise alignment during implantation is critical; even slight rotation can reduce the astigmatism-correcting benefit. Toric models are available in both monofocal and premium multifocal configurations, giving patients with astigmatism broader options for their target vision outcome.
Light Adjustable Lens
A light adjustable lens (LAL) is an intraocular lens whose optical power can be fine-tuned after cataract surgery using targeted ultraviolet light treatments. The surgeon adjusts the lens prescription during follow-up visits based on how the eye has healed, allowing a level of postoperative customization that fixed IOLs cannot offer. This approach may benefit patients who want the most precise refractive outcome possible, including those with prior LASIK or complex prescriptions. Once the desired correction is achieved, a final UV lock-in treatment stabilizes the lens permanently.
With the right IOL selected, preparing properly before surgery helps ensure the best possible outcome.
How Should You Prepare Before Cataract Surgery?
You should prepare before cataract surgery by completing a pre-operative eye exam, adjusting medications, and arranging logistics for surgery day.
What Happens During the Pre-Operative Eye Exam?
The pre-operative eye exam is a comprehensive evaluation your ophthalmologist performs one to two weeks before cataract surgery. This exam serves two purposes: confirming the health of your eye and collecting precise measurements for your intraocular lens (IOL).
During this appointment, your surgeon’s team typically performs:
- Biometry measurements to determine the correct IOL power for your eye.
- Corneal topography to map the shape of your cornea and detect astigmatism.
- Pupil dilation to examine the retina and optic nerve for any underlying conditions.
- Ocular surface assessment to identify dry eye or other surface issues that could affect surgical outcomes.
Accurate biometry is arguably the single most important factor in achieving a good refractive result, so patients should not rush through this step. If you wear contact lenses, your doctor may ask you to stop wearing them several days before the exam to ensure accurate corneal readings.
What Medications Should You Stop Before Cataract Surgery?
The medications you should stop before cataract surgery typically include blood thinners and certain prostate medications, though changes depend on your surgeon’s specific instructions. According to the American Academy of Ophthalmology, your surgical team will review your full medication list during preoperative planning.
Common medication adjustments include:
- Blood thinners (such as warfarin or aspirin) may need to be paused or continued depending on your cardiovascular risk.
- Alpha-blockers like tamsulosin can cause intraoperative floppy iris syndrome, so your surgeon needs advance notice.
- Anticoagulant eye drops or supplements with blood-thinning properties may require temporary discontinuation.
Never stop any medication without direct guidance from both your eye surgeon and prescribing physician. This coordination between providers is essential for patient safety, yet it remains one of the most commonly overlooked steps in surgical preparation.
What Should You Arrange for the Day of Surgery?
You should arrange transportation, fasting compliance, and a comfortable post-operative setup for the day of surgery. Cataract surgery is an outpatient procedure, so planning ahead eliminates unnecessary stress.
Key logistics to organize include:
- A responsible driver to take you home, since you cannot drive yourself after receiving sedation or dilating drops.
- Fasting for at least 6 to 8 hours before the procedure if your surgeon requires it, typically no food or drink after midnight.
- Comfortable, loose clothing and avoidance of facial cosmetics, perfumes, or lotions on surgery day.
- Prescribed eye drops ready at home so you can begin your post-operative regimen immediately.
Arriving 30 to 60 minutes early allows time for pre-surgical prep, including additional dilating drops and a final review with your anesthesia team. Having these arrangements settled in advance lets you focus entirely on a smooth surgical experience and recovery.
What Happens During the Cataract Surgery Procedure?
The cataract surgery procedure involves local anesthesia, a short operative time, and a precise sequence of surgical steps. The sections below cover anesthesia type, procedure duration, and the step-by-step stages.
What Type of Anesthesia Is Used for Cataract Surgery?
The type of anesthesia used for cataract surgery is typically topical anesthesia, delivered as numbing eye drops applied directly to the eye’s surface. This approach eliminates pain while allowing the patient to remain awake and responsive throughout the procedure. In some cases, a local anesthetic injection (peribulbar or retrobulbar block) may be administered around the eye for additional numbing, particularly when longer or more complex surgery is anticipated.
A mild sedative given intravenously can help patients feel calm and relaxed during the operation. General anesthesia is rarely required and is typically reserved for patients who cannot cooperate due to anxiety, involuntary movement disorders, or other medical considerations. Most patients report feeling little to no discomfort, with only mild pressure sensations during the procedure.
How Long Does the Cataract Surgery Procedure Take?
The cataract surgery procedure typically takes between 10 and 30 minutes for uncomplicated cases, with the majority completed in approximately 15 minutes. This short duration reflects the procedure’s high degree of refinement. According to a 2025 report published by JAMA, cataract surgery is one of the most common procedures in high-income countries, with more than 3.5 million operations performed annually in the United States.
Several factors can influence total operative time, including cataract density, the surgical technique used, and whether additional procedures are performed simultaneously. Although the surgery itself is brief, patients should expect to spend two to three hours at the surgical facility to account for pre-operative preparation, anesthesia administration, and post-operative monitoring before discharge.
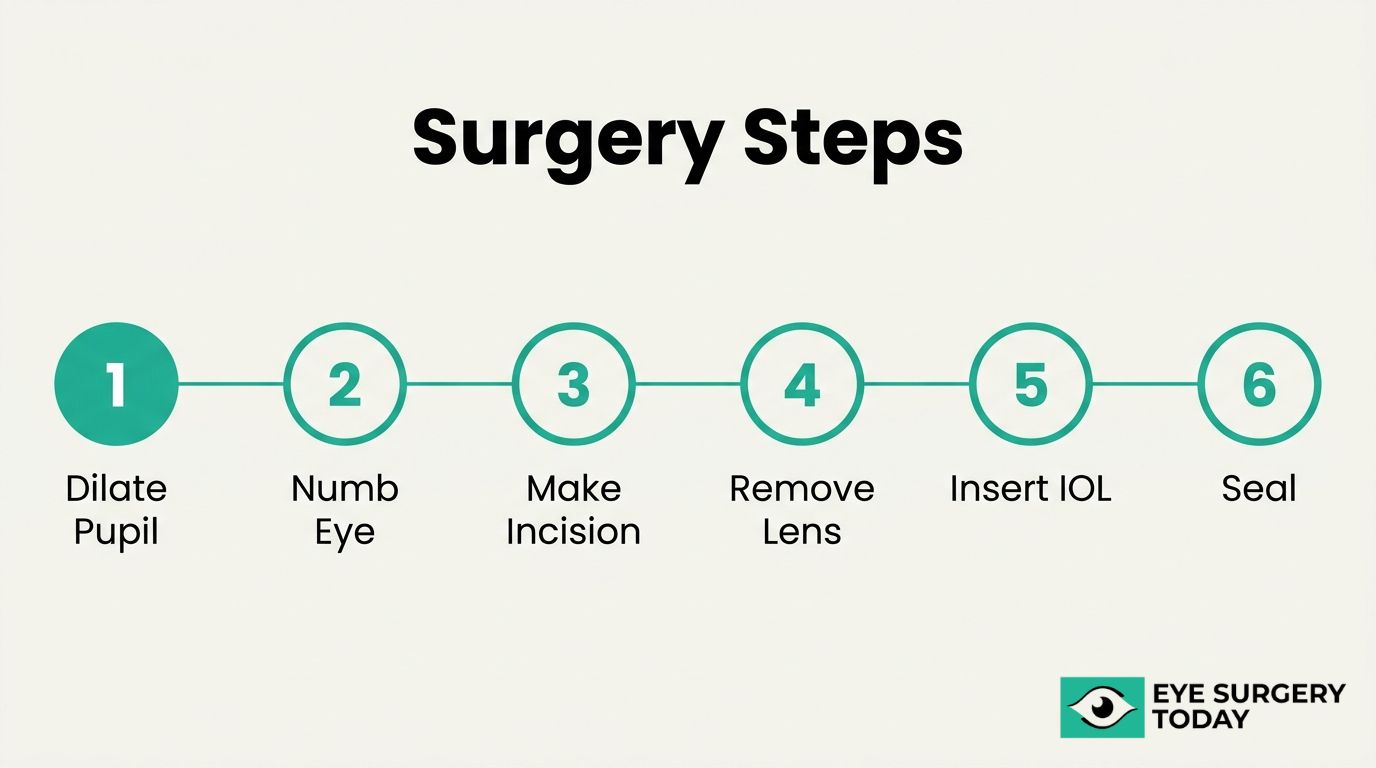
What Are the Step-by-Step Stages of Cataract Surgery?
The step-by-step stages of cataract surgery follow a precise, standardized sequence:
- Pupil dilation. Medicated eye drops widen the pupil to give the surgeon a clear view of the lens.
- Anesthesia application. Topical numbing drops (or a local injection) are administered to ensure the eye is completely pain-free.
- Corneal incision. The surgeon creates a small incision, typically 2 to 3 millimeters, at the edge of the cornea.
- Capsulotomy. A circular opening is made in the anterior capsule, the thin membrane surrounding the natural lens.
- Lens removal. Using phacoemulsification, an ultrasound probe breaks the cloudy lens into fragments, which are then suctioned out of the eye.
- IOL implantation. A folded intraocular lens is inserted through the same small incision and positioned inside the remaining lens capsule, where it unfolds into place.
- Incision sealing. The micro-incision is typically self-sealing and often requires no sutures.
The entire sequence is performed under an operating microscope, giving the surgeon magnified precision at every stage. Understanding these steps before surgery day can help reduce anxiety and set realistic expectations for the experience.
What Should You Expect During Cataract Surgery Recovery?
Cataract surgery recovery follows a predictable timeline, with most improvements occurring within the first few weeks. The sections below cover what to expect in the first 24 hours, the first week, the first month, and when vision fully stabilizes.

What Should You Expect in the First 24 Hours After Surgery?
In the first 24 hours after surgery, you should expect mild discomfort, blurry vision, and light sensitivity as your eye begins its initial healing. A protective eye shield is typically placed over the operated eye immediately after the procedure, and your ophthalmologist may recommend wearing it while sleeping to prevent accidental rubbing or pressure.
Common experiences during this period include:
- Watery or slightly bloodshot appearance in the treated eye.
- A gritty or itchy sensation that gradually subsides.
- Mild grogginess from sedation used during the procedure.
- Sensitivity to bright lights, making sunglasses helpful outdoors.
Your surgeon will prescribe antibiotic and anti-inflammatory eye drops, usually starting the same day. Patients are generally advised not to drive for at least 24 hours after cataract surgery, according to Optegra Eye Health Care. Resting quietly and avoiding screens for extended periods can help minimize strain during this critical early window.
What Should You Expect in the First Week After Surgery?
In the first week after surgery, you should expect gradual visual improvement alongside continued use of prescribed eye drops. While many patients notice clearer vision within a few days, some fluctuation in sharpness and contrast is normal as the eye adjusts to the new intraocular lens.
Key guidelines for the first week include:
- Attending your follow-up appointment, typically scheduled one to two days after surgery.
- Continuing antibiotic and anti-inflammatory drops on the prescribed schedule.
- Avoiding heavy lifting, bending at the waist, and strenuous activity.
- Keeping water, soap, and shampoo away from the operated eye during bathing.
Some patients experience mild halos or glare around lights at night; this usually diminishes as healing progresses. In most cases, the first week represents the steepest curve of visual recovery, so patience during this phase is essential.
What Should You Expect in the First Month After Surgery?
In the first month after surgery, you should expect your vision to continue stabilizing as internal healing completes. Most patients resume their normal daily routines within two to three weeks, though your ophthalmologist may advise continued caution with certain activities.
During this period, residual symptoms typically resolve:
- Mild dryness or intermittent blurriness decreases steadily.
- Light sensitivity fades as the eye fully adapts to the implanted lens.
- Eye drop regimens are gradually tapered based on healing progress.
A follow-up visit around the one-month mark allows your surgeon to assess healing and determine whether a new glasses prescription is needed. For patients who had both eyes treated on different dates, the second eye procedure is often scheduled during this window. Staying consistent with drop schedules and protecting the eye from dust or debris supports the best possible outcome.
When Is Vision Fully Stabilized After Cataract Surgery?
Vision is fully stabilized after cataract surgery within approximately four to eight weeks for most patients. According to Best Cataract Surgeons, full recovery generally takes four to eight weeks, by which time 90% of patients have achieved their final visual outcome.
Several factors can influence the exact timeline:
- The type of intraocular lens implanted, as multifocal or extended depth of focus lenses may require a longer neuroadaptation period.
- Pre-existing conditions, such as diabetic retinopathy or macular degeneration, which can affect how quickly vision settles.
- The health of the cornea and overall ocular surface at the time of surgery.
Once vision stabilizes, your eye care provider will finalize any updated prescription for glasses or reading lenses. Most patients find that their best corrected vision after surgery represents a significant improvement over their pre-surgical baseline. Understanding that full stabilization is a weeks-long process helps set realistic expectations from the start.
What Activities Should You Avoid After Cataract Surgery?
You should avoid driving, strenuous exercise, heavy lifting, and exposing your eye to water or dust during the initial recovery period. The sections below cover specific timelines for driving, work, exercise, showering, and flying.
How Soon Can You Drive After Cataract Surgery?
You can typically drive after cataract surgery once your ophthalmologist confirms adequate visual acuity, which often occurs within 24 to 48 hours. According to Optegra Eye Health Care, patients are typically advised not to drive for at least 24 hours after cataract surgery. Several factors may extend this timeline:
- Residual blurriness or light sensitivity on the day after surgery
- Use of sedation that may impair reaction time
- Difficulty with depth perception if only one eye has been treated
Your eye care provider will assess your vision at the first postoperative visit before clearing you to drive. Waiting for that confirmation, rather than self-assessing, is the safest approach.
How Soon Can You Return to Work After Cataract Surgery?
You can return to work after cataract surgery within a few days for most desk-based or low-impact jobs. Patients with physically demanding occupations that involve heavy lifting, exposure to dust, or bright outdoor environments may need to wait one to two weeks before resuming full duties.
- Office or remote work: often possible within 1 to 3 days
- Light retail or service roles: typically safe after 3 to 5 days
- Construction, manufacturing, or outdoor labor: usually requires 1 to 2 weeks
Prolonged screen time can contribute to eye strain during early recovery, so taking frequent breaks and using lubricating drops as directed may help ease the transition. Your surgeon’s clearance should guide the final decision.
How Soon Can You Exercise After Cataract Surgery?
You can exercise after cataract surgery on a graduated timeline, starting with light walking within the first day or two. Patients are generally advised to avoid strenuous activity or heavy lifting for the first week postoperatively, as increased intraocular pressure from straining can interfere with healing.
A practical return-to-exercise timeline includes:
- Days 1 to 3: Gentle walking at a comfortable pace
- Week 1 to 2: Light yoga, stationary cycling, or moderate-paced walking
- Week 2 to 4: Gradual return to weight training, jogging, and gym workouts
- After 4 weeks: Full-intensity exercise, contact sports, and swimming
Activities involving water exposure, such as swimming or hot tubs, carry a higher risk of introducing bacteria to the healing eye. Most surgeons consider waiting at least four weeks for these activities to be a reasonable precaution.
How Soon Can You Shower or Wash Your Hair After Surgery?
You can shower after surgery within the first 24 hours, but you should take precautions to prevent water, soap, or shampoo from entering the operated eye. Full recovery after cataract surgery generally takes 4 to 8 weeks, so protecting the eye from irritants during the early healing phase is essential.
Helpful precautions during the first one to two weeks include:
- Keeping your eyes closed while rinsing your hair
- Tilting your head backward so water flows away from the face
- Avoiding direct water pressure on or near the eye
- Using a clean, damp washcloth around the eye area instead of splashing water
Most surgeons allow normal face washing and hair care after the first week, though care should still be taken to avoid rubbing the eye.
How Soon Can You Fly After Cataract Surgery?
You can fly after cataract surgery within a few days in most uncomplicated cases, though many ophthalmologists recommend waiting at least one week. Cabin pressure changes during air travel do not typically affect the eye after standard cataract surgery because the procedure does not introduce gas into the eye.
Situations that may require a longer wait before flying include:
- Concurrent retinal procedures involving intraocular gas bubbles
- Unresolved postoperative inflammation or elevated eye pressure
- Inability to attend a follow-up appointment before departure
Carrying lubricating eye drops on the flight can help counteract the dry cabin air that often worsens postoperative dryness. Confirming clearance with your surgeon before booking travel ensures the safest timeline for your specific recovery.
With activity restrictions understood, knowing the potential risks and complications of cataract surgery helps you recognize warning signs early.
What Are the Possible Risks and Complications?
The possible risks and complications of cataract surgery include posterior capsule opacification, infection, cystoid macular edema, and retinal detachment. The following subsections cover each complication and the warning signs that require prompt medical attention.
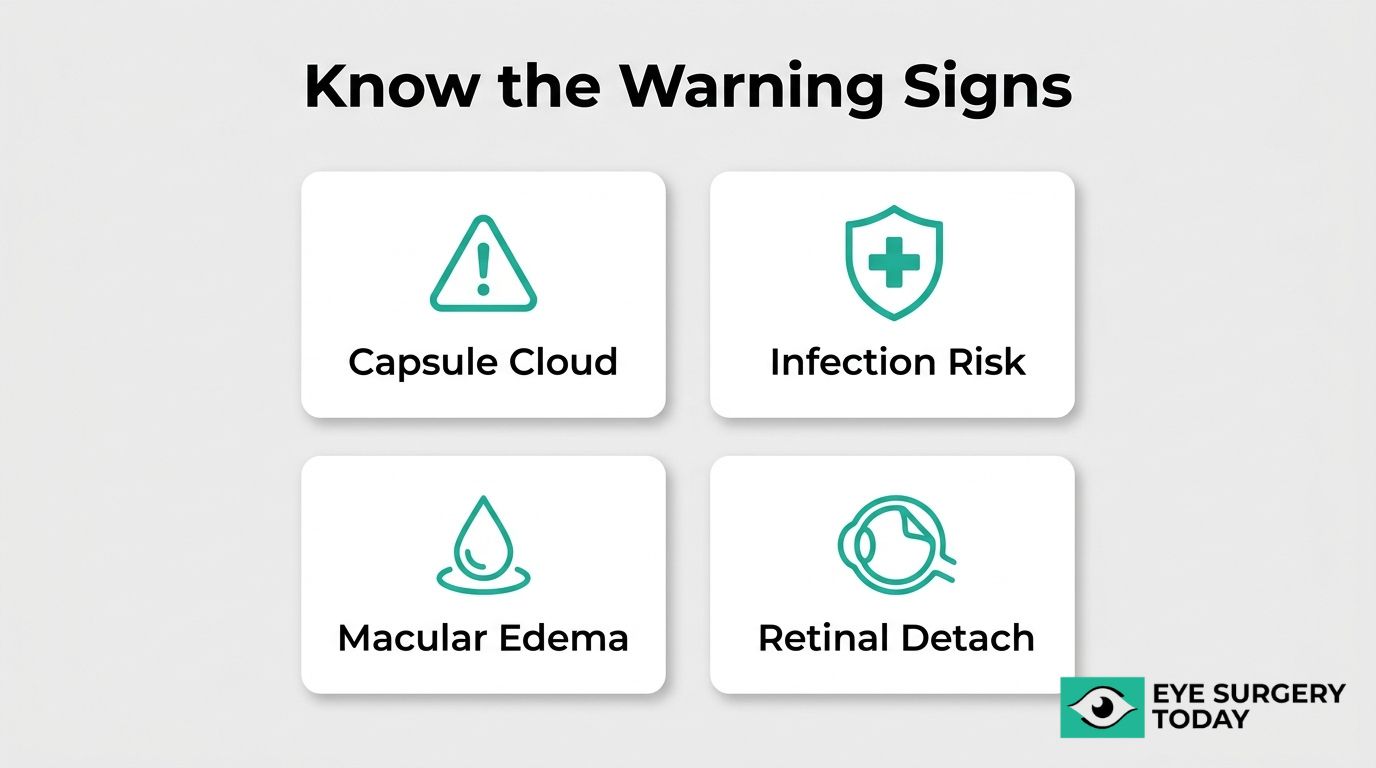
What Is Posterior Capsule Opacification?
Posterior capsule opacification (PCO) is a gradual clouding of the thin membrane left behind the intraocular lens after cataract surgery. PCO develops when residual lens epithelial cells proliferate across the posterior capsule, causing blurred or hazy vision that can resemble the original cataract symptoms. According to research from Sri Devaraj Urs Academy of Higher Education and Research, PCO remains the most common complication following cataract surgery.
A quick, painless outpatient procedure called YAG laser capsulotomy can treat PCO. The laser creates a small opening in the clouded capsule, restoring clear vision within days for most patients. Because PCO may develop months or even years after the initial surgery, routine follow-up appointments play an important role in early detection.
What Is the Risk of Infection After Cataract Surgery?
The risk of infection after cataract surgery is very low, though endophthalmitis remains the most serious infectious complication. This condition involves bacterial or fungal organisms entering the eye during or shortly after the procedure.
According to a report published in JAMA, the use of intraoperative intraocular antibiotics, such as moxifloxacin or cefuroxime, has reduced the rate of sight-threatening postsurgical endophthalmitis from 0.07% to 0.02%. Modern sterile techniques and prophylactic antibiotic protocols have made this complication rare, yet its potential severity is why surgeons emphasize strict post-operative hygiene. Touching the eye, skipping prescribed antibiotic drops, or exposing the eye to contaminated water in the early recovery period can increase infection risk.
What Is Cystoid Macular Edema After Cataract Surgery?
Cystoid macular edema (CME) after cataract surgery is a condition where fluid-filled cysts accumulate in the macula, the central part of the retina responsible for sharp vision. CME can cause blurred or distorted central vision, typically appearing several weeks after the procedure.
Patients with pre-existing conditions may face elevated risk. As noted by the American Academy of Ophthalmology, proper planning and management of the ocular surface are essential for patients with comorbid glaucoma or diabetic macular edema, since ocular surface disease is common in these populations and can affect surgical outcomes. Anti-inflammatory eye drops, including NSAIDs and corticosteroids, are the standard treatment for post-surgical CME. Most cases resolve with consistent medication use, though persistent edema may require additional intervention.
Can Retinal Detachment Occur After Cataract Surgery?
Yes, retinal detachment can occur after cataract surgery, although it is uncommon. Retinal detachment happens when the retina separates from the underlying supportive tissue, potentially leading to permanent vision loss if untreated.
Certain factors may increase this risk:
- High myopia (severe nearsightedness) before surgery.
- A history of retinal detachment in either eye.
- Surgical complications during the cataract procedure, such as posterior capsule rupture.
- Younger patient age at the time of surgery.
Symptoms typically include a sudden increase in floaters, flashes of light, or a shadow spreading across the visual field. Because retinal detachment is a medical emergency, anyone experiencing these symptoms after cataract surgery should seek immediate evaluation.
What Are the Signs You Should Call Your Doctor?
The signs you should call your doctor after cataract surgery include any symptom that suggests a complication is developing. Contact your ophthalmologist promptly if you experience:
- Sudden, significant vision loss or worsening blurriness.
- Increasing eye pain that does not improve with prescribed medication.
- Intense redness that spreads or worsens after the first few days.
- New flashes of light or a sudden shower of floaters.
- A dark curtain or shadow moving across your field of vision.
- Persistent swelling or discharge from the eye.
Most post-operative discomfort is mild and resolves within days. However, any rapid change in vision or escalating pain warrants urgent attention, as early treatment of complications like infection or retinal detachment can be critical for preserving sight. Understanding these risks helps patients approach their recovery with both confidence and appropriate vigilance.
How Much Does Cataract Surgery Typically Cost?
Cataract surgery cost depends on insurance coverage and lens selection. Medicare, private insurance, and premium lens upgrades each affect the final price differently.
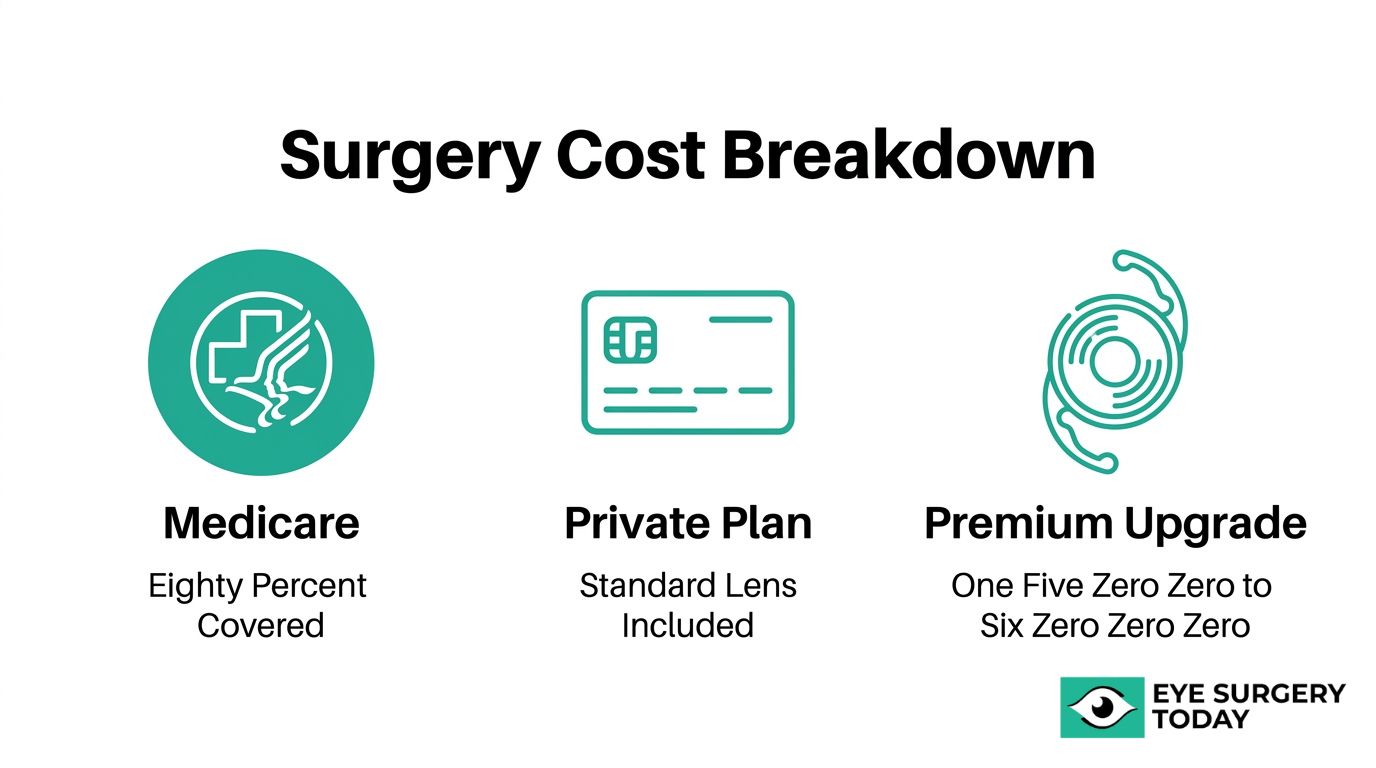
Does Medicare Cover Cataract Surgery?
Medicare covers cataract surgery when the procedure is deemed medically necessary. Medicare Part B typically pays 80% of the approved costs once the annual deductible has been met, leaving patients responsible for the remaining 20% coinsurance. In 2026, that annual deductible is $283, according to data reported by The Big 65.
Supplemental Medigap policies or Medicare Advantage plans can reduce or eliminate that 20% coinsurance, making the out-of-pocket expense significantly lower for many beneficiaries. Standard monofocal intraocular lenses are included in Medicare’s approved amount, though upgrades to premium lenses typically require additional patient payment. For most patients on Medicare, cataract surgery remains one of the more affordable surgical procedures, especially when supplemental coverage is in place.
Does Private Insurance Cover Cataract Surgery?
Private insurance covers cataract surgery in most cases when a physician documents that cataracts impair daily functioning. Coverage typically includes the surgeon’s fee, facility costs, anesthesia, and a standard monofocal IOL. Patients should verify their specific plan’s deductible, copay, and any prior authorization requirements before scheduling.
Where private insurance falls short is with advanced technology lenses. According to a 2024 report published in JAMA, advanced technology IOLs, such as multifocal or extended depth of focus designs, can reduce dependence on eyeglasses but involve additional out-of-pocket costs not covered by standard medical insurance. The gap between what insurance approves and what premium lenses cost is the primary source of unexpected expenses for privately insured patients.
What Is the Out-of-Pocket Cost for Premium Lens Upgrades?
The out-of-pocket cost for premium lens upgrades typically ranges from $1,500 to $6,000 per eye, based on 2026 estimates from Pacific Eye. This amount covers the difference between a standard monofocal IOL, which insurance or Medicare includes, and an advanced technology lens.
Several factors influence the final price:
- Lens type selected: Multifocal, extended depth of focus, toric, and light adjustable lenses each carry different surcharges.
- Advanced diagnostic testing: Measurements such as optical biometry or corneal topography may add to the total.
- Facility and geographic variation: Costs differ between ambulatory surgery centers and hospital-based settings.
Because these upgrades are considered elective, neither Medicare nor most private insurers reimburse the added expense. Patients weighing premium lenses should request an itemized cost breakdown before surgery to avoid surprises.
Understanding cost and coverage is one part of preparing for cataract surgery; knowing what results to realistically expect is equally important.
What Results Can Cataract Surgery Potentially Achieve?
Cataract surgery can potentially achieve significant improvements in visual acuity, reduced dependence on corrective eyewear, and enhanced quality of life. The specific results depend on factors such as the type of intraocular lens implanted, the patient’s overall eye health, and the presence of any coexisting conditions.
Most patients experience noticeably clearer vision within days of the procedure, though full visual stabilization may take several weeks. According to JAMA, cataract surgery is one of the most commonly performed procedures in high-income countries, with more than 3.5 million operations completed annually in the U.S. as of 2025; this volume reflects consistently high success rates and patient satisfaction. The Centers for Medicare & Medicaid Services tracks patient satisfaction within 90 days following cataract surgery as a formal quality indicator, and most patients consistently achieve high levels of satisfaction through careful perioperative management. Many types of eye surgery contribute to improved quality of life, including functional or cosmetic eyelid surgery.
Beyond sharper distance vision, enhanced monofocal IOLs and advanced technology lenses may help improve intermediate and near vision, potentially reducing the need for reading glasses. Patients with astigmatism who receive toric IOLs can also experience meaningful correction of pre-existing refractive error. While individual outcomes vary, cataract surgery remains one of the safest and most predictable procedures in modern medicine, and for most patients, the improvement in daily visual function is substantial.
How Does Cataract Surgery Compare to Living With Cataracts?
Cataract surgery compares to living with cataracts as a decisive intervention that may restore functional vision, whereas untreated cataracts progressively worsen over time. Cataracts cannot reverse on their own; no eye drops, medications, or lifestyle changes can eliminate the clouding once it develops. The only definitive treatment is surgical removal of the opaque lens and replacement with an artificial intraocular lens.
Living with cataracts means adapting to a gradual decline in visual clarity. Early cataracts may cause mild blurriness, increased glare sensitivity, and faded color perception. As the condition advances, these symptoms can intensify to the point where everyday tasks, such as reading, driving at night, and recognizing faces, become increasingly difficult. For some individuals, this progressive vision loss may contribute to reduced independence and a higher risk of falls.
Cataract surgery, by contrast, is one of the most frequently performed procedures in high-income countries. According to a 2025 report published in JAMA, more than 3.5 million cataract operations are performed annually in the United States alone. Full recovery generally takes four to eight weeks, and the majority of patients experience meaningful improvement in visual function. While every surgical procedure carries some degree of risk, modern techniques and intraoperative antibiotics have reduced serious complications to very low rates.
From a practical standpoint, the choice often comes down to timing. When cataracts begin interfering with daily activities or quality of life, surgery typically offers a far better long-term outcome than continued adaptation. Delaying surgery is safe when symptoms remain mild, but waiting until cataracts become very advanced can sometimes make the procedure more complex. Discussing the right timing with an eye care provider helps ensure the best balance between managing symptoms and achieving optimal surgical results.
How Can Surgeon-Reviewed Resources Help You Prepare for Cataract Surgery?
Surgeon-reviewed resources can help you prepare for cataract surgery by providing clinically accurate, easy-to-understand information about every stage of the process. For parents whose children require ophthalmic intervention, understanding infant cataract surgery success rates is particularly vital for navigating care options. The sections below cover how Eye Surgery Today supports informed decision-making and the essential takeaways from this guide.
Can Eye Surgery Today Help You Understand Your Options?
Yes, Eye Surgery Today can help you understand your options by offering surgeon-reviewed educational content that covers cataract surgery techniques, intraocular lens choices, recovery expectations, cost considerations, and congenital cataracts. The platform was built by nationally recognized ophthalmology key opinion leaders to bridge the gap between complex clinical knowledge and patient understanding.
Every guide and resource on Eye Surgery Today is reviewed by practicing surgeons, ensuring the information reflects current evidence-based practice. Topics range from candidacy criteria for patients with glaucoma, diabetes, or prior LASIK to detailed comparisons of monofocal, multifocal, toric, and extended depth of focus IOLs. Rather than replacing a conversation with your eye doctor, these resources prepare you to ask better questions and evaluate your choices with greater confidence. For patients navigating a procedure performed over 3.5 million times annually in the United States, having access to unbiased, surgeon-reviewed information can make the difference between uncertainty and clarity.
What Are the Key Takeaways About Cataract Surgery?
The key takeaways about cataract surgery are that it is a safe, well-established procedure with high patient satisfaction and a recovery period that typically spans four to eight weeks. The most important points to remember include:
- Cataract surgery removes the clouded natural lens and replaces it with an artificial intraocular lens, usually in 10 to 30 minutes.
- Candidacy depends on individual eye health; conditions such as glaucoma, diabetes, prior LASIK, or pediatric cataracts require specialized planning but do not necessarily disqualify you.
- IOL selection directly affects your post-surgical vision, with options ranging from standard monofocal lenses to premium multifocal, EDOF, toric, and light adjustable lenses.
- Most patients can resume daily activities within days, though full visual stabilization may take several weeks.
- Medicare Part B typically covers 80% of approved surgical costs after the annual deductible, while premium lens upgrades involve additional out-of-pocket expense.
- Rare complications, such as posterior capsule opacification or infection, are treatable when caught early.
Preparing thoroughly and consulting surgeon-reviewed resources, like those on Eye Surgery Today, can help you approach cataract surgery with confidence and realistic expectations.





