An eye exam for cataracts is a specialized diagnostic evaluation that assesses lens clarity, visual function, and overall eye health to determine whether a cataract is present, how it affects daily vision, and whether surgical intervention may be appropriate.
This guide covers the diagnostic tests involved in a comprehensive cataract exam, specialized imaging and measurement tools used for surgical planning, the distinct cataract types each exam can identify, screening guidelines based on age and risk factors, and the decision-making process from diagnosis through surgery.
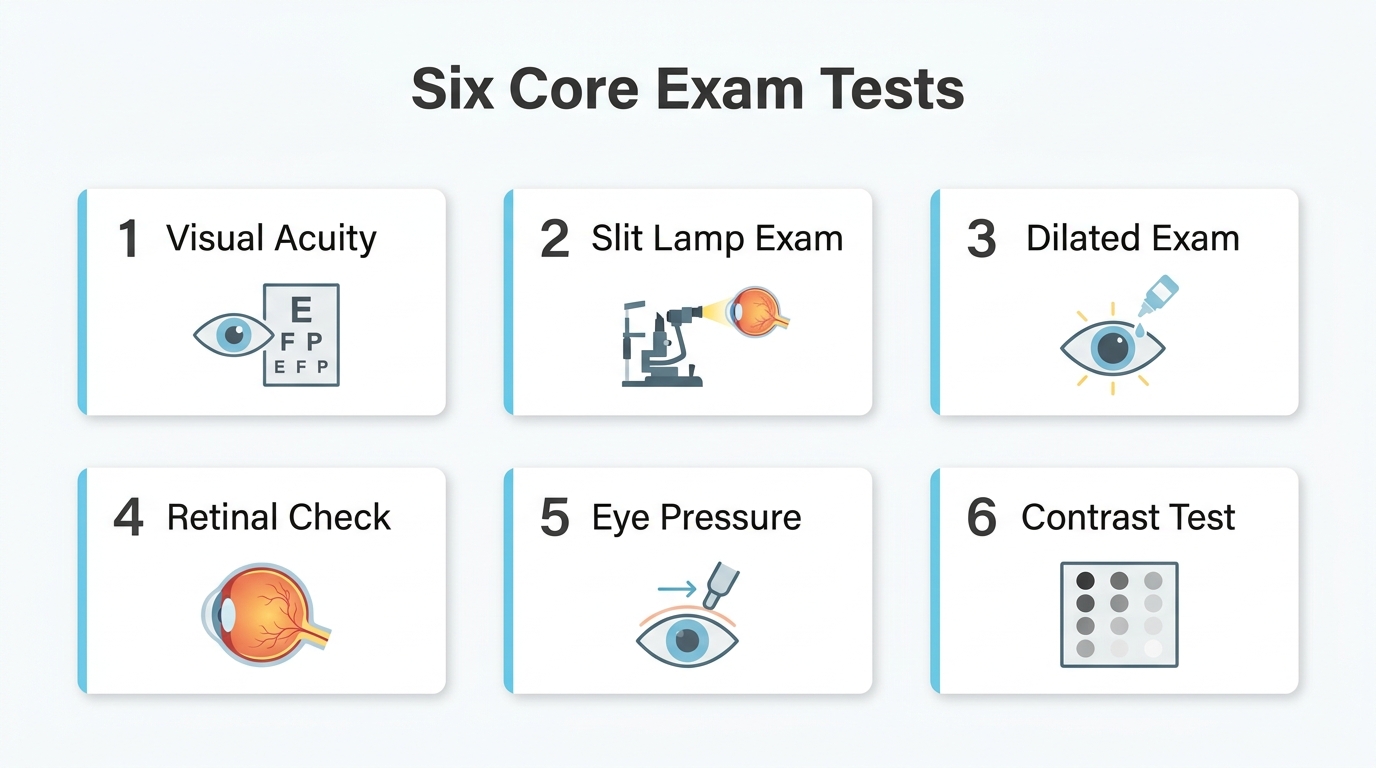
A comprehensive cataract exam combines several core tests, including visual acuity measurement, slit-lamp biomicroscopy, dilated fundus evaluation, tonometry, contrast sensitivity assessment, and refraction. Each test contributes a distinct piece of information; visual acuity establishes a baseline, while contrast sensitivity and glare testing may capture functional deficits that standard acuity charts miss.
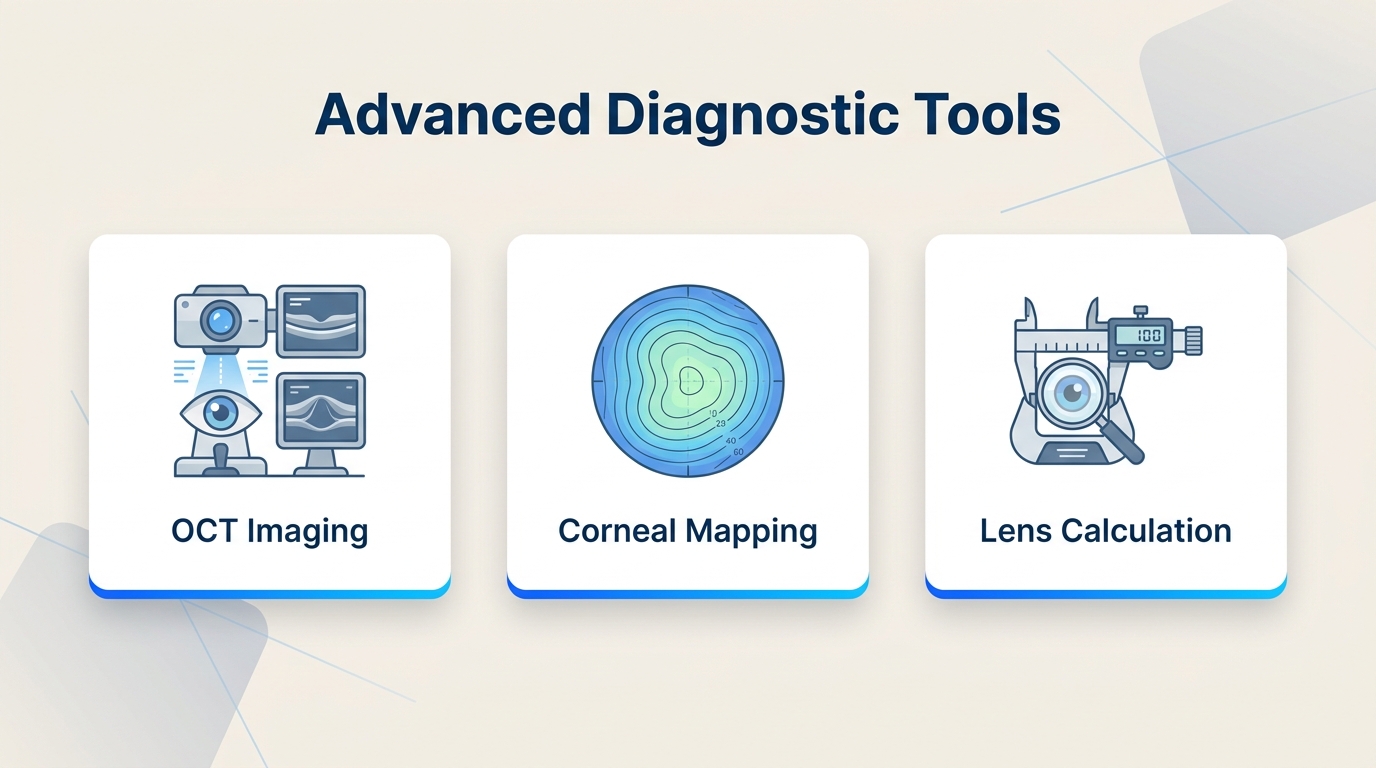
Beyond standard diagnostics, specialized tools such as optical coherence tomography, corneal topography, optical biometry, and specular microscopy help ophthalmologists evaluate retinal health, map corneal curvature, measure axial length for intraocular lens calculations, and assess corneal endothelial cell integrity before surgery.
Cataracts vary by location within the lens and by cause. Nuclear sclerotic, cortical, posterior subcapsular, congenital, traumatic, and secondary cataracts each produce distinct visual symptoms and diagnostic patterns that guide treatment planning.
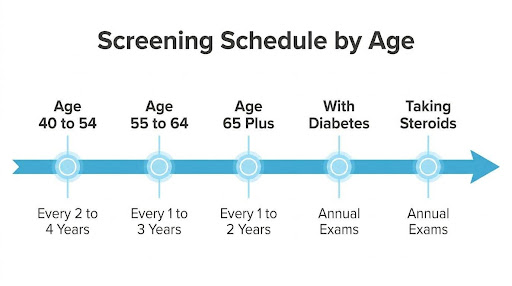
Screening frequency depends on age and individual risk. Adults 40 to 54 without risk factors may need exams every two to four years, while adults 55 to 64 generally benefit from one to three year evaluation.
Grading systems such as LOCS III translate exam findings into standardized severity scores, and the decision to proceed with surgery is based on how the cataract affects daily vision and quality of life rather than on acuity scores alone.
What Happens During a Comprehensive Eye Exam for Cataracts?
A comprehensive eye exam for cataracts involves a series of diagnostic tests that evaluate lens clarity, overall eye health, and visual function. The following sub-sections cover each core test.
What Does the Visual Acuity Test Measure?
The visual acuity test measures the clarity and sharpness of your vision at specific distances. According to the American Academy of Ophthalmology, visual acuity in the clinic is typically measured at distance using a Snellen chart to assess how well you can distinguish letters or symbols at various distances.
This test establishes a baseline reading, often expressed as a fraction like 20/20 or 20/40. However, visual acuity scores alone do not determine whether cataract surgery is appropriate. The National Institute for Health and Care Excellence (NICE) states that access to cataract surgery should not be restricted on the basis of visual acuity alone; the decision should instead reflect how the cataract affects the person’s daily vision and quality of life. A patient with moderate acuity loss but significant difficulty driving at night, for instance, may be a stronger surgical candidate than someone with lower scores who functions well in daily tasks.
What Does the Slit-Lamp Examination Reveal?
The slit-lamp examination reveals detailed structural information about the front portions of the eye, including the cornea, iris, and lens. This biomicroscope projects a thin, focused beam of light while the ophthalmologist views magnified cross-sections of each structure.
Cataracts become visible under slit-lamp illumination as areas of cloudiness or discoloration within the lens. The examiner can determine whether the opacity sits in the nucleus, cortex, or posterior capsule, which helps classify the cataract type. Corneal irregularities and anterior chamber abnormalities are also assessed during this step, since these findings may influence surgical planning. For many clinicians, the slit-lamp exam is the single most informative component when evaluating early lens changes that other tests might miss.
How Does a Dilated Eye Exam Help Detect Cataracts?
A dilated eye exam helps detect cataracts by widening the pupil with special drops, giving the ophthalmologist an unobstructed view of the entire lens and the structures behind it. Without dilation, only a limited central portion of the lens is visible.
Once the pupil is fully dilated, the examiner uses a fundus lens, direct ophthalmoscope, or indirect ophthalmoscope to evaluate the retina and posterior segment. This broader field of view allows detection of lens opacities that may be located at the periphery or rear surface of the lens. Dilation also enables assessment of the retina and optic nerve, which is critical because conditions like macular degeneration or diabetic retinopathy can coexist with cataracts and affect treatment decisions.
What Does the Retinal Exam Check For?
The retinal exam checks for abnormalities in the retina, optic nerve, and blood vessels at the back of the eye. These structures are evaluated after dilation to confirm that the retina is healthy enough to benefit from cataract surgery.
Conditions such as macular degeneration, diabetic retinopathy, and retinal detachment can be identified during this examination. If significant retinal disease is present, it may limit the visual improvement achievable through cataract removal alone. The ophthalmologist uses this information to set realistic outcome expectations and determine whether additional treatments are needed before or alongside surgery. A thorough retinal evaluation is essential because a perfectly clear artificial lens cannot restore vision compromised by underlying retinal damage.
How Does Tonometry Screen for Other Conditions?
Tonometry screens for other conditions by measuring intraocular pressure (IOP), which is the fluid pressure inside the eye. Elevated IOP is the primary risk factor for glaucoma, a condition that can cause irreversible optic nerve damage.
During tonometry, either a small puff of air or a gentle contact probe is applied to the corneal surface to obtain a pressure reading. Normal IOP typically ranges between 10 and 21 mmHg. When elevated pressure is detected alongside cataract findings, the ophthalmologist can coordinate a treatment plan that addresses both conditions. This screening step matters because glaucoma and cataracts frequently coexist in older adults, and identifying both early allows for more comprehensive surgical planning.
What Does the Contrast Sensitivity Test Evaluate?
The contrast sensitivity test evaluates your ability to distinguish objects from their background at varying levels of contrast. While standard acuity charts use high-contrast black letters on white backgrounds, real-world vision often demands recognizing low-contrast details.
According to Aetna’s clinical policy guidelines, pre-operative cataract testing includes contrast sensitivity testing, glare testing, potential vision testing, and specular photographic microscopy to assess endothelial cells. Reduced contrast sensitivity is one of the earliest functional symptoms of cataracts, often appearing before significant acuity loss on a Snellen chart. Patients who struggle with night driving or reading in dim lighting frequently show measurable deficits on this test, making it a valuable tool for capturing the true functional impact of a developing cataract.
What Role Does Refraction Play in a Cataract Exam?
Refraction plays a central role in a cataract exam by determining the precise optical prescription needed for clearest possible vision. The ophthalmologist uses a phoropter or trial lenses to identify the degree of nearsightedness, farsightedness, or astigmatism present.
In cataract evaluation, refraction serves a dual purpose. First, it reveals whether vision loss can be corrected with updated glasses or whether the cataract itself is the primary cause of blurred vision. Second, refractive measurements guide intraocular lens (IOL) power selection if surgery is recommended. Shifts in refraction over time, particularly a sudden increase in nearsightedness known as “second sight,” can indicate nuclear cataract progression. Accurate refraction data is foundational to achieving the best visual outcome after lens replacement.
With each of these tests contributing a distinct piece of diagnostic information, specialized imaging and measurement tools can provide even deeper evaluation of the cataract.
What Specialized Tests Are Used to Evaluate Cataracts?
Specialized tests used to evaluate cataracts include optical coherence tomography, corneal topography, A-scan ultrasound biometry, IOLMaster measurements, specular microscopy, and potential acuity testing.
What Does Optical Coherence Tomography Show?
Optical coherence tomography (OCT) shows detailed cross-sectional images of the retina, macula, and optic nerve. This non-invasive imaging test uses light waves to capture high-resolution scans of each retinal layer, revealing conditions that a cataract may be masking.
Before cataract surgery, OCT can detect macular degeneration, diabetic macular edema, epiretinal membranes, or macular holes that could limit visual improvement after lens replacement. If the retina appears compromised on OCT, the surgeon can set realistic expectations for postoperative vision. Ophthalmologists rely on OCT as a baseline assessment tool because cataracts alone do not always explain the full extent of vision loss.
How Does Corneal Topography Assist Cataract Evaluation?
Corneal topography assists cataract evaluation by mapping the curvature and shape of the cornea’s surface. The device projects light rings onto the cornea and generates a color-coded topographic map that highlights irregularities, steep zones, and flat areas.
This mapping is essential for several pre-surgical decisions:
- Identifying pre-existing astigmatism that may require a toric intraocular lens.
- Detecting irregular corneal conditions, such as keratoconus, that could affect surgical outcomes.
- Guiding incision placement to minimize surgically induced astigmatism.
Without accurate topography data, selecting the optimal IOL type and power becomes significantly less precise. For patients considering premium lens implants, this test is particularly valuable. Precise corneal measurements are also foundational for planning advanced procedures like laser cataract surgery, which can enhance accuracy in incision creation and astigmatism correction.
What Does an A-Scan Ultrasound Biometry Measure?
A-scan ultrasound biometry measures the axial length of the eye, which is the distance from the cornea to the retina. This measurement is critical for calculating the correct intraocular lens power before cataract surgery.
According to the National Institute for Health and Care Excellence (NICE), optical biometry is the preferred method for measuring axial length, with ultrasound biometry used as a secondary option when optical measurements are not possible. Dense cataracts can block the light signal used in optical devices, making ultrasound the necessary alternative. The probe contacts the cornea through a thin layer of coupling fluid, and the resulting measurement directly influences refractive accuracy after surgery.
What Is the IOLMaster and How Is It Used?
The IOLMaster is a non-contact optical biometry device used to measure key ocular dimensions for intraocular lens calculation. It captures axial length, anterior chamber depth, corneal curvature, and white-to-white corneal diameter in a single session.
Because the IOLMaster uses partial coherence interferometry rather than ultrasound, no corneal contact is required. This makes the measurement process faster and more comfortable. The device feeds its data directly into IOL power formulas, helping surgeons select the lens that best matches the patient’s target refraction. When a cataract is too dense for light-based measurement, clinicians switch to A-scan ultrasound as the backup method.
How Does Specular Microscopy Assess Corneal Health?
Specular microscopy assesses corneal health by photographing and analyzing the endothelial cell layer on the inner surface of the cornea. These cells maintain corneal clarity by pumping excess fluid out of the corneal stroma.
The test measures three key indicators:
- Cell density: the number of endothelial cells per square millimeter.
- Cell morphology: variations in cell size (polymegethism) and shape (pleomorphism).
- Overall endothelial function: predicting the cornea’s ability to recover after surgical stress.
A low endothelial cell count before cataract surgery may indicate increased risk of postoperative corneal swelling or decompensation. Identifying compromised corneal endothelium in advance allows the surgeon to modify the surgical technique and counsel the patient appropriately.
What Does Potential Acuity Testing Predict?
Potential acuity testing predicts the best visual acuity a patient may achieve after cataract removal. The test projects a small visual acuity chart directly onto the retina, bypassing the clouded lens entirely.
If the projected image yields good acuity readings, the retina and optic nerve are likely healthy enough to benefit from surgery. Conversely, poor results may suggest underlying macular disease or optic neuropathy that would limit postoperative improvement. This distinction is valuable when a dense cataract prevents adequate retinal examination through standard methods. For patients and surgeons alike, potential acuity testing provides a practical forecast that shapes both surgical expectations and the decision to proceed. In some cases, simulating post-surgical vision outcomes with special contact lenses can further aid patient understanding and decision-making.
With specialized testing complete, grading the cataract’s severity guides the next clinical steps.
What Are the Different Types of Cataracts an Exam Can Identify?
The different types of cataracts an exam can identify include nuclear sclerotic, cortical, posterior subcapsular, congenital, traumatic, and secondary cataracts. Each type forms in a distinct part of the lens and produces unique visual symptoms.
Nuclear Sclerotic Cataracts
Nuclear sclerotic cataracts are the most common age-related cataract type. They form in the central zone of the lens, known as the nucleus. As the eye ages, it adds new lens fibers that compress the nucleus over time, gradually hardening and yellowing the core. According to StatPearls (National Center for Biotechnology Information), nuclear cataracts have an incidence of 13.1%, making them the most frequently diagnosed age-related variety. Early stages may temporarily improve near vision, a phenomenon sometimes called “second sight,” before distance vision progressively worsens. Because changes develop slowly, many patients do not notice significant symptoms until the cataract reaches moderate density. This gradual onset makes routine comprehensive eye exams especially valuable for early detection.
Cortical Cataracts
Cortical cataracts affect the outer layer of the lens, known as the cortex. These cataracts develop as white, wedge-shaped opacities called “cortical spokes” that extend from the periphery toward the center of the lens. Glare and difficulty with contrast are common early complaints, particularly when driving at night. As the spokes progress inward, they increasingly scatter incoming light and interfere with both distance and near vision. Patients with diabetes or prolonged ultraviolet light exposure may face a higher likelihood of developing cortical opacities. A slit-lamp examination is especially effective at revealing these spoke-like changes before they reach the visual axis.
Posterior Subcapsular Cataracts
Posterior subcapsular cataracts form on the back surface of the lens capsule, directly in the path of light entering the eye. These cataracts can cause paradoxical vision symptoms: patients may experience poor vision in bright lighting conditions yet improved vision in dim lighting, as reported by Gelman Vision. This occurs because bright light constricts the pupil, forcing light through the central opacity, while dim light dilates the pupil and allows light around the cataract. Posterior subcapsular cataracts tend to progress faster than other types. Long-term corticosteroid use and high myopia are recognized contributing factors, making this type particularly important to monitor in at-risk populations.
Congenital Cataracts
Congenital cataracts are present at birth or develop during early infancy. According to Practice Plus Group, parents or pediatricians can often recognize congenital cataracts through an asymmetrical red reflex or by noticing the infant’s failure to track light sources. Causes may include genetic inheritance, intrauterine infections, or metabolic disorders. Early detection is critical because the developing visual system requires clear optical input during the first months of life. Without timely intervention, congenital cataracts can lead to amblyopia, a condition where the brain favors one eye over the other. Pediatric ophthalmologists typically recommend prompt evaluation when any lens opacity is suspected in a newborn.
Traumatic Cataracts
Traumatic cataracts develop after physical injury to the eye. Blunt force, penetrating wounds, chemical burns, or radiation exposure can damage the lens fibers and trigger cataract formation. Symptoms may appear immediately following the injury or develop months to years later, depending on the severity and type of trauma. The opacity pattern often differs from age-related cataracts, sometimes appearing as a rosette or stellate shape visible on slit-lamp examination. Younger patients involved in sports, industrial work, or accidents represent the most common demographic. A thorough eye exam after any significant ocular trauma is essential, even when initial vision seems unaffected.
Secondary Cataracts
Secondary cataracts develop as a consequence of another medical condition, medication, or prior eye surgery. Diabetes, prolonged corticosteroid use, and previous intraocular procedures are among the most common contributing factors. The American Academy of Ophthalmology Preferred Practice Pattern notes that smoking is a significant risk factor for various types of cataracts, and patients should be counseled regarding the risk of cataract development from tobacco use. Secondary cataracts may also refer to posterior capsule opacification, which can occur after cataract surgery when residual lens cells proliferate on the capsule. In clinical practice, distinguishing secondary cataracts from primary types is important because managing the underlying cause often influences both treatment timing and surgical planning.
Understanding each cataract type helps clarify how exam results guide the next steps in your care.
How Should You Prepare for a Cataract Eye Exam?
You should prepare for a cataract eye exam by gathering your medical history, adjusting medications as directed, and arranging transportation home after pupil dilation.
- Bring a complete medication list. Include all prescription drugs, over-the-counter supplements, and eye drops you currently use. Your ophthalmologist needs this information to assess risk factors, such as long-term corticosteroid use, which is an established contributor to early cataract development.
- Note your current vision complaints. Write down specific situations where your vision feels impaired, such as difficulty driving at night, increased glare sensitivity, or trouble reading. These details help your doctor evaluate how the cataract affects your daily quality of life.
- Bring your current eyeglasses or contact lenses. Your provider will compare your existing prescription against new measurements taken during the exam.
- Arrange a driver for after the appointment. Dilating drops blur near vision and increase light sensitivity for several hours, making it unsafe to drive immediately afterward.
- Ask about medication adjustments beforehand. Certain blood thinners or alpha-blockers may need to be discussed with your prescribing physician before specific cataract tests.
- Prepare questions about your diagnosis. Knowing what to ask, such as the type and severity of your cataract or the timeline for follow-up, helps you leave the appointment with a clear understanding of next steps.
Arriving prepared allows your ophthalmologist to conduct a thorough evaluation and provide the most accurate recommendations. With a clear picture of your cataract, the next step is recognizing the symptoms that prompted the exam in the first place.
What Symptoms May Prompt Your Doctor to Test for Cataracts?
The symptoms that may prompt your doctor to test for cataracts include blurred or cloudy vision, increased glare sensitivity, difficulty seeing at night, fading colors, and frequent changes in eyeglass prescriptions. These warning signs often develop gradually, making regular eye exams essential for early detection.
Blurred vision is typically the earliest and most common complaint. As the lens becomes increasingly opaque, images lose sharpness at both near and far distances. This differs from simple refractive error because the blur may not fully correct with new glasses.
Increased sensitivity to glare, particularly from headlights or bright sunlight, can signal lens changes that scatter incoming light. Posterior subcapsular cataracts can cause paradoxical vision symptoms, where patients experience poor vision in good lighting but improved vision in dim lighting, according to Gelman Vision. This pattern often catches patients off guard.
Other symptoms that may lead to cataract testing include:
- Double vision in one eye, caused by irregular light refraction through the cloudy lens.
- A noticeable yellowing or browning of colors, especially in nuclear cataracts.
- Needing brighter light for reading or close-up tasks.
- Frequent prescription changes that no longer improve clarity.
- Halos appearing around lights, particularly at night.
In clinical practice, the combination of symptoms matters more than any single complaint. A patient reporting both glare sensitivity and color shift, for instance, presents a stronger indication for targeted cataract evaluation than someone with mild blur alone. Many of these symptoms overlap with other eye conditions, which is precisely why a comprehensive cataract exam, rather than self-diagnosis, remains critical for accurate identification.
Understanding these early warning signs helps patients seek timely evaluation before vision loss affects daily activities and quality of life.
Who Should Get Screened for Cataracts and How Often?
Cataract screening frequency depends on age and risk factors. The sections below cover recommended exam intervals for adults under 55, adults 55 to 64, adults 65 and older, people with diabetes, and people on long-term steroids.
How Often Should Adults Under 55 Get Screened?
Adults under 55 should get screened for cataracts every two to four years, starting at age 40. This baseline exam allows an ophthalmologist to detect early lens changes before symptoms appear.
According to an American Academy of Ophthalmology clinical statement, individuals without risk factors aged 40 to 54 should be examined by an ophthalmologist every two to four years. Those with risk factors, such as a family history of cataracts, UV exposure, or smoking, may need more frequent evaluations. Even without noticeable vision changes, early-stage opacities can develop silently during this period. Establishing a screening baseline in your 40s gives your eye doctor a reference point for tracking any progression over time.
How Often Should Adults Between 55 and 64 Get Screened?
Adults between 55 and 64 should get screened for cataracts every one to three years. Lens changes accelerate during this decade, making shorter intervals between exams important for early detection.
Age-related nuclear sclerosis becomes increasingly common with age, and subtle shifts in contrast sensitivity or night vision often go unnoticed without a comprehensive dilated exam. Even patients who feel their vision is adequate may benefit from closer monitoring, since cataracts at this stage can progress unevenly between eyes. For most people in this age group without additional risk factors, a one-to-three-year cycle strikes the right balance between vigilance and practicality.
How Often Should Adults 65 and Older Get Screened?
Adults 65 and older should get screened for cataracts every year. Cataract prevalence rises sharply after 65, and annual exams help ophthalmologists identify visually significant changes before they impair daily function.
At this stage, screening also evaluates for concurrent conditions, such as glaucoma and macular degeneration, that can complicate cataract management. Because lens opacities may worsen gradually, patients sometimes adapt to diminished vision without realizing the extent of decline. Routine exams catch these changes early, preserving options for surgical timing. For adults over 65, consistent screening is one of the most reliable ways to protect both visual quality and overall safety.
How Often Should People with Diabetes Get Screened?
People with diabetes should get screened for cataracts at least once every year. Diabetes accelerates cataract formation, and annual dilated exams allow ophthalmologists to monitor both lens clarity and retinal health simultaneously.
According to a study published in PubMed Central (National Institutes of Health), patients with cataracts and diabetes mellitus tend to be older, have a longer duration of diabetes, and exhibit poorer metabolic control compared to those without cataracts. This connection means tighter screening intervals are essential, particularly for patients with poorly controlled blood sugar. Annual exams also help detect diabetic retinopathy, which can influence surgical planning and intraocular lens selection if cataract removal becomes necessary.
How Often Should People on Long-Term Steroids Get Screened?
People on long-term steroids should get screened for cataracts per their ophthalmologist’s recommended schedule. Long-term corticosteroid use is an established risk factor for early cataract development, particularly posterior subcapsular cataracts.
Steroid-induced lens changes can progress faster than typical age-related cataracts, sometimes appearing within months of sustained use. Patients taking oral, inhaled, or topical corticosteroids for conditions such as asthma, autoimmune disorders, or chronic inflammation should discuss screening frequency with their eye doctor. Because these cataracts tend to affect the back of the lens, they may cause disproportionate glare and reading difficulty early on. Proactive annual monitoring ensures timely intervention before significant vision loss occurs.
With a clear screening schedule in place, the next step is understanding how exam results are used to grade cataract severity.
How Are Cataract Exam Results Used to Grade Severity?
Cataract exam results are used to grade severity through standardized classification systems that measure lens opacity across multiple dimensions. The most widely used system is LOCS III.
Ophthalmologists rely on the LOCS III (Lens Opacities Classification System III) grading scale to translate subjective exam findings into consistent, comparable severity scores. According to a study published in PubMed (National Library of Medicine), the LOCS III cataract grading system enhances the ability of surgeons to estimate ultrasonic energy expenditure and balanced salt solution volume use during phacoemulsification.
LOCS III grades cataracts based on four parameters:
- Nuclear color: The degree of yellowing or browning within the lens nucleus.
- Nuclear opalescence: The level of whitish cloudiness in the central lens fibers.
- Cortical changes: The extent and location of spoke-like opacities in the outer lens cortex.
- Posterior subcapsular opacification: The density of clouding on the back surface of the lens capsule.
Each parameter receives a numeric score compared against standardized reference photographs, giving clinicians a reproducible measure of cataract progression. This structured approach removes much of the guesswork from clinical assessments, allowing different providers to communicate about the same patient’s condition with shared terminology.
What makes LOCS III particularly valuable in practice is that grading does not simply label a cataract as “mild” or “severe.” Instead, it provides granular data that directly informs surgical planning. Higher nuclear opalescence scores, for instance, signal a denser lens that may require more phacoemulsification energy during extraction. Surgeons use this information to anticipate procedure complexity and select appropriate techniques before entering the operating room.
Grading results also help determine whether a patient’s visual symptoms align with the degree of lens opacity observed on examination. With severity properly classified, the next step involves determining what happens after a formal cataract diagnosis.
What Happens After a Cataract Is Diagnosed?
After a cataract is diagnosed, your ophthalmologist develops a personalized management plan based on the cataract’s type, severity, and its impact on your daily vision. This plan may range from monitoring and lifestyle adjustments to pre-surgical testing and intraocular lens selection.
Once a diagnosis is confirmed, the next steps typically include:
- Establishing a baseline grade using a standardized system to track progression over time.
- Assessing functional impact on activities such as driving, reading, and working in varied lighting.
- Discussing monitoring intervals for early-stage cataracts that do not yet require intervention.
- Ordering pre-operative testing if surgery is appropriate, including optical biometry and corneal evaluation.
- Selecting an intraocular lens (IOL) matched to the patient’s visual goals and eye health profile.
According to the National Institute for Health and Care Excellence (NICE), access to cataract surgery should not be restricted on the basis of visual acuity alone; instead, the decision should be based on how the cataract affects the person’s vision and quality of life. This patient-centered approach means two individuals with identical acuity scores may follow very different timelines. In clinical practice, this nuance is often underappreciated, yet it is one of the most important factors in achieving meaningful visual outcomes after surgery.
Temporary measures, such as updated eyeglass prescriptions, anti-glare coatings, or brighter task lighting, can help manage symptoms while the cataract is monitored. These strategies do not slow cataract progression, but they may preserve functional independence during the observation period.
Understanding what follows a diagnosis helps patients feel more prepared when discussing surgical timing and lens options with their eye care team. Part of this preparation includes discussing the likelihood of possible glasses use after surgery, even with advanced IOLs, to ensure expectations align with potential visual outcomes.
How Can You Tell When Cataracts Require Surgery?
You can tell when cataracts require surgery by evaluating how significantly they impair your daily vision and quality of life, not by visual acuity scores alone.
Cataract surgery is not triggered by a single test result. The decision involves a complex clinical evaluation that weighs multiple factors together. Your ophthalmologist considers the severity of your symptoms, your diagnostic data, and the potential risks of the procedure before recommending surgery.
According to the American Academy of Ophthalmology, medical decision-making for cataract surgery requires meeting high complexity levels in at least two of three components: the patient’s problem, the data reviewed, and the risk of complications. This means no universal threshold exists; what qualifies one patient for surgery may not apply to another.
Key indicators your ophthalmologist may evaluate include:
- Difficulty performing daily activities, such as driving, reading, or working, despite updated prescriptions.
- Glare or halos around lights that interfere with nighttime driving safety.
- Reduced contrast sensitivity confirmed through specialized testing.
- A cataract grade severe enough to affect visual function as measured by standardized grading systems.
- Failure of non-surgical options, such as stronger glasses or magnification, to restore adequate vision.
The timing of cataract surgery is ultimately a shared decision between you and your eye care provider. In clinical practice, the most reliable signal is functional impairment: when the cataract prevents you from living the way you want to, despite conservative measures, surgery becomes a reasonable next step. Patients who wait for a specific acuity number often delay unnecessarily, while those who communicate their real-world limitations tend to receive more timely, personalized care.
Understanding when surgery is warranted helps frame the consequences of postponing evaluation altogether.
What Are the Possible Risks of Delaying a Cataract Exam?
The possible risks of delaying a cataract exam include undetected progression of lens opacity, increased surgical complexity, and preventable vision loss that may affect daily safety and independence.
Cataracts are a progressive condition, meaning the lens continues to cloud over time regardless of whether symptoms feel manageable. When an exam is postponed, the ophthalmologist loses the opportunity to establish a baseline grade of cataract severity, track the rate of change, and identify the optimal window for intervention. What begins as mild blurriness can gradually advance to a stage where driving, reading, and recognizing faces become difficult.
A more mature cataract also changes the surgical landscape. Dense, advanced cataracts may require higher ultrasonic energy during phacoemulsification, which can increase stress on the corneal endothelium and raise the risk of post-operative complications. Early detection through a timely exam allows the surgeon to plan a less complex procedure with more predictable outcomes.
Beyond the cataract itself, a comprehensive cataract exam can reveal other conditions, such as glaucoma, diabetic retinopathy, or macular degeneration, that may otherwise remain undiagnosed. According to the World Health Organization, cataracts affect more than 94 million people globally and remain the leading cause of remediable blindness worldwide. Much of that burden is concentrated in populations with limited access to routine screening, underscoring how a delayed exam can turn a treatable condition into permanent vision loss.
From a clinical perspective, the cost of waiting is almost always higher than the cost of an early exam. Patients who monitor cataracts from an early stage benefit from a wider range of intraocular lens options and more predictable refractive results after surgery. Delaying that first evaluation removes those advantages and narrows the path to the best possible visual outcome.
How Does a Cataract Eye Exam Differ from a Routine Eye Exam?
A cataract eye exam differs from a routine eye exam in scope, diagnostic tools, and clinical purpose. While both assess overall eye health, a cataract-focused evaluation adds specialized tests that measure lens opacity, visual function under specific conditions, and surgical planning data. With global cataract cases surging from 32.8 million in 1990 to over 82 million in 2021 according to a study published in the Nature Eye Journal, the clinical distinction between these two exam types has become increasingly relevant for patients and providers alike.
A routine comprehensive eye exam typically includes visual acuity measurement, refraction for corrective lens prescriptions, tonometry for intraocular pressure, and a general assessment of ocular structures. These exams screen for common conditions and update prescriptions. For instance, routine eye exams can also uncover other ophthalmic issues, such as those that might lead to eyelid surgery for functional or cosmetic reasons. A cataract eye exam incorporates all of these elements but extends significantly further, layering in targeted diagnostics designed to characterize the cataract, evaluate its impact on daily function, and determine surgical readiness.
Key differences between a cataract eye exam and a routine eye exam include:
- Lens-focused slit-lamp evaluation: A routine exam uses slit-lamp biomicroscopy broadly, while a cataract exam specifically grades lens opacity, location, and type.
- Contrast sensitivity and glare testing: These tests quantify how the cataract affects functional vision beyond what a standard acuity chart reveals.
- Dilated fundus examination depth: Both exams may include dilation, but a cataract evaluation examines the retina and posterior segment more thoroughly to rule out conditions that could limit surgical outcomes.
- Biometry and IOL calculations: Cataract exams include axial length measurement and corneal curvature mapping for intraocular lens selection, which routine exams never require.
- Potential acuity testing: This predicts post-surgical visual potential, a step with no equivalent in a standard screening visit.
In clinical practice, the most overlooked distinction is intent. A routine exam answers the question “how healthy are your eyes today?” while a cataract exam answers “how is this cataract affecting your life, and what will surgery need to correct?” That shift in clinical reasoning drives every additional test in the cataract workup. Understanding this difference helps patients recognize why their ophthalmologist may recommend a more detailed evaluation when cataracts are suspected or progressing.
How Can Informed Patients Approach Cataract Surgery Decisions?
Informed patients can approach cataract surgery decisions by understanding their exam results, asking about lens options, and knowing what to expect on surgery day. The sections below cover how Eye Surgery Today supports that process and the key takeaways from this guide.
Can Eye Surgery Today Help You Understand Your Options?
Yes, Eye Surgery Today can help you understand your options by providing educational content on cataract surgery, intraocular lens selection, and what to expect before, during, and after the procedure. As an education platform founded by nationally recognized ophthalmology KOLs, Eye Surgery Today translates complex surgical information into clear, accessible guidance.
Choosing the right intraocular lens (IOL) is one of the most consequential decisions in the cataract surgery process. Toric IOLs, for example, are specifically designed to correct astigmatism during cataract surgery, providing clearer distance vision and reducing the need for spectacles, according to the American Academy of Ophthalmology. Understanding the differences between monofocal, multifocal, toric, and extended depth of focus lenses requires reliable, unbiased information. Eye Surgery Today offers educational articles, surgeon profiles, and decision-making guides that help patients navigate these choices with confidence. In my experience, patients who arrive at their surgical consultation already informed about IOL categories tend to have more productive conversations with their surgeon and feel more satisfied with their outcomes.
What Are the Key Takeaways About Eye Exams for Cataracts?
The key takeaways about eye exams for cataracts are that early detection, thorough diagnostic testing, and informed decision-making form the foundation of effective cataract care.
- A comprehensive cataract eye exam includes visual acuity testing, slit-lamp examination, dilated fundus evaluation, tonometry, and contrast sensitivity assessment.
- Specialized pre-surgical tests, such as optical biometry, corneal topography, and specular microscopy, help ophthalmologists plan precise IOL selection and surgical approach.
- Cataract types, including nuclear sclerotic, cortical, posterior subcapsular, and congenital, each present distinct diagnostic features that exams are designed to identify.
- Screening frequency should follow age-based and risk-based guidelines, with more frequent exams for patients over 55, those with diabetes, and individuals on long-term corticosteroids.
- Surgery decisions should be based on how the cataract affects vision and quality of life, not visual acuity scores alone.
According to NICE guidelines, patients must be informed of their position on the surgical list and what to expect during and immediately after the procedure on the day of surgery. Proactive, informed patients consistently achieve better outcomes because they understand both the diagnostic process and their treatment options before entering the operating room. This understanding extends to the importance of ongoing eye wellness after the procedure, ensuring long-term vision protection.





