Biometry is the measurement of key anatomical dimensions of the eye, including axial length, corneal curvature, anterior chamber depth, and lens thickness, used to calculate intraocular lens (IOL) power before cataract surgery. This guide covers what biometry measures, how IOL power is determined, the biological and technical factors that limit precision, refractive surprises and their management, the role of prior LASIK or PRK, current measurement technologies, and strategies surgeons use to improve accuracy.
Each eye measurement feeds into mathematical formulas that predict the ideal lens strength. Modern formulas like Barrett Universal II and Hill-RBF 3.0 incorporate more anatomical variables and artificial intelligence than earlier generations, narrowing the gap between predicted and actual outcomes.
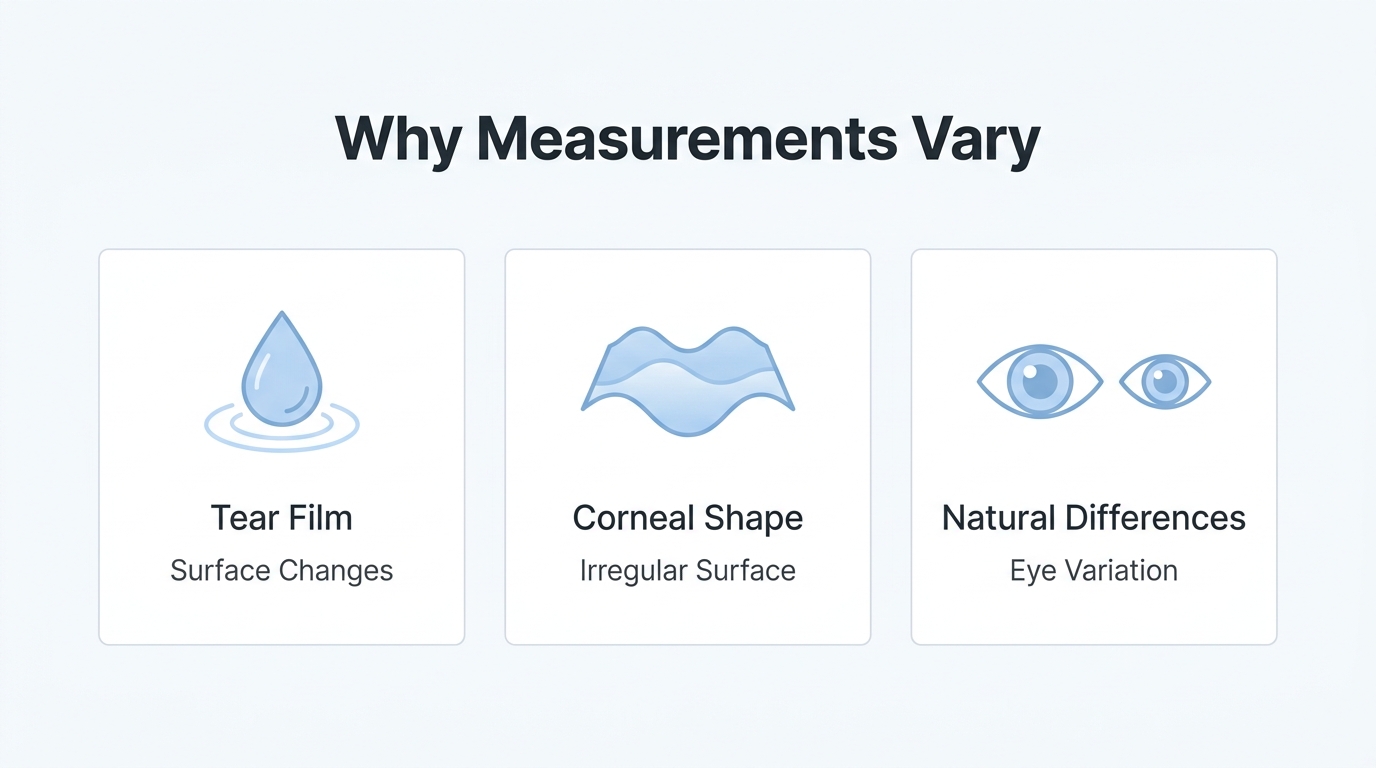
Living eyes introduce variability that no instrument can fully eliminate. Tear film instability, corneal surface irregularities, and natural differences in internal dimensions between patients all contribute small measurement uncertainties that can compound through IOL calculations. Very long or very short eyes amplify these effects further.
A refractive surprise occurs when the postoperative outcome differs from the intended target. While the majority of eyes in standard cataract surgery land close to the predicted result, options ranging from updated prescriptions to laser enhancements exist when the outcome falls outside expectations. Prior corneal refractive surgery adds complexity by altering the cornea’s natural curvature, requiring specialized formulas to compensate.
Optical biometry, contact ultrasound, and immersion ultrasound each serve distinct clinical roles depending on a patient’s eye conditions. Surgeons further reduce error through repeated measurements, intraoperative aberrometry, and thorough preoperative patient education that sets realistic expectations about what biometry can achieve.
What Does Biometry Measure in the Eye?
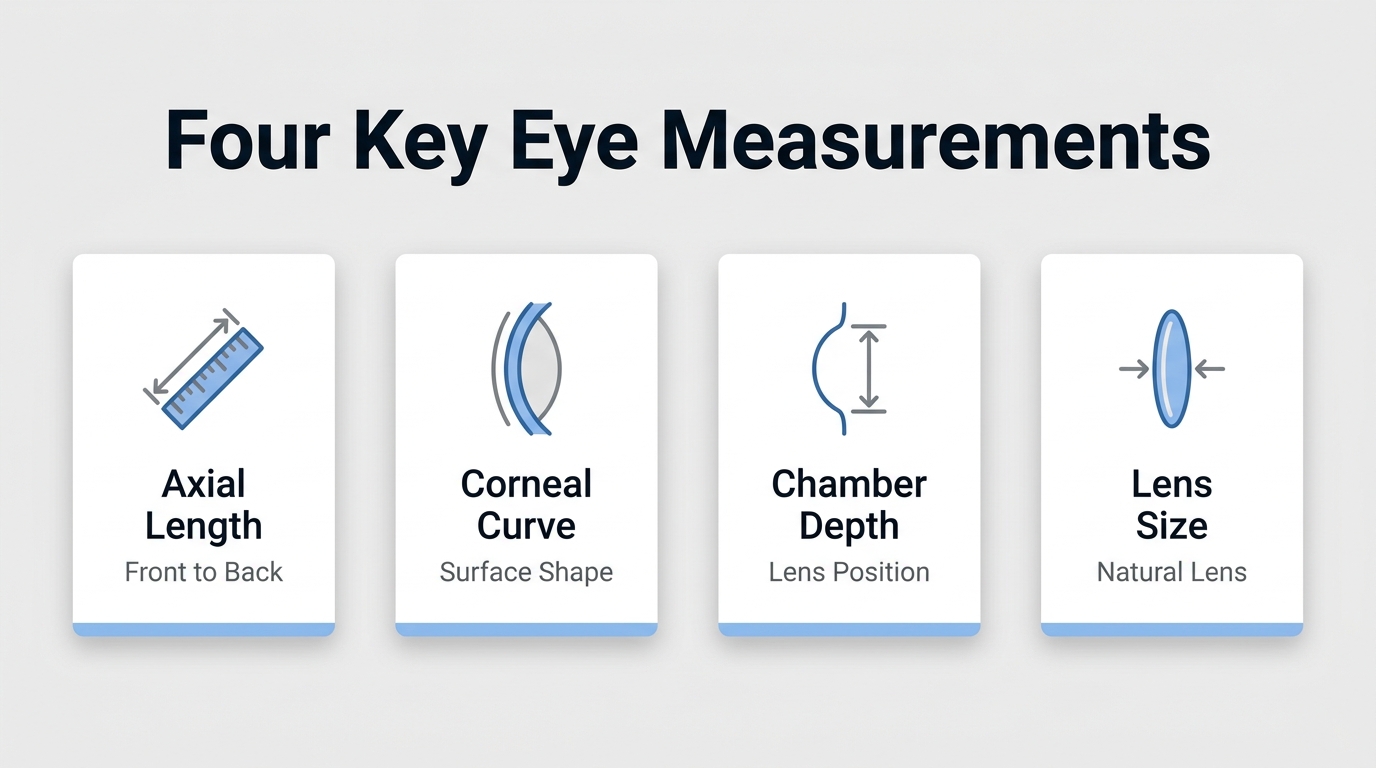
Biometry measures the anatomical dimensions of the eye, including axial length, corneal curvature, anterior chamber depth, and lens thickness. Each measurement feeds directly into the formula that determines IOL power before cataract surgery.
How Is Axial Length Measured During Biometry?
Axial length is measured during biometry using either optical or ultrasound methods to determine the distance from the anterior corneal surface to the retinal pigment epithelium. Optical biometry uses light instead of sound, producing more accurate results because ultrasound wavelengths are many times longer. Optical devices also incorporate the actual thickness of the retina, whereas ultrasound adds a standard 200 micrometers to the axial length reading.
When ultrasound is necessary, the immersion technique tends to yield longer, more reliable measurements than the contact method, which can introduce subjective errors from corneal compression. Even with optical devices, ocular surface conditions matter. According to a 2022 study published on ResearchGate, tear film instability and corneal surface irregularity are important sources of variability in keratometric and axial length measurements in cataract patients. Clinicians should also be aware that artificial tears can affect readings, so waiting at least five minutes after installation is generally recommended before performing biometry.
How Does Biometry Measure Corneal Curvature?
Biometry measures corneal curvature through keratometry, which quantifies the steepness of the front surface of the cornea in diopters or millimeters of radius. According to StatPearls (NCBI), ocular biometry refers to the measurement of anatomical dimensions of the eye, which include corneal curvature, axial length, and anterior chamber depth. Modern optical biometers capture multiple data points across the corneal surface, providing a detailed map rather than a single average value.
Because even minor keratometric errors can shift the IOL power calculation, accurate corneal curvature data is essential. Dry eye disease, in particular, may reduce measurement repeatability by disrupting the tear film that the device reads through. This is why many surgeons treat ocular surface disease before finalizing biometry readings.
How Is Anterior Chamber Depth Assessed?
Anterior chamber depth is assessed by measuring the distance from the posterior corneal surface to the anterior surface of the crystalline lens. According to a 2024 study published in PMC (National Institutes of Health), the anterior segment length is defined as the sum of the anterior chamber depth and lens thickness. This relationship helps IOL formulas estimate where the implant will sit after surgery, a value known as effective lens position.
Shallow anterior chambers, often found in hyperopic eyes, can make this prediction more challenging. Accurate ACD measurement contributes meaningfully to reducing postoperative refractive error, which is why modern biometers capture it alongside axial length and keratometry in a single automated scan.
What Role Does Lens Thickness Play in Biometry?
Lens thickness plays a critical role in biometry because it directly influences the prediction of effective lens position after cataract surgery. According to the Moran Eye Center at the University of Utah, lens thickness is the distance between the anterior and posterior lens surfaces and is an important determinant of effective lens position, measured in millimeters.
Thicker lenses, which are common in older patients with advanced cataracts, can shift the predicted IOL position and alter the power calculation. Newer-generation IOL formulas incorporate lens thickness as a variable, improving accuracy over older formulas that ignored it entirely. For patients who have previously undergone corneal refractive surgery, intraoperative wavefront aberrometry may further refine outcomes by verifying lens power in real time.
Understanding these four core measurements helps explain both the precision biometry can achieve and why small errors in any single parameter can compound during IOL calculation.
How Does Biometry Determine IOL Power?
Biometry determines IOL power by feeding precise eye measurements into mathematical formulas that predict the ideal lens strength. The subsections below cover how these formulas work and how modern versions improve upon older generations.
What Are IOL Calculation Formulas?
IOL calculation formulas are mathematical models that convert biometry measurements into a recommended intraocular lens power for cataract surgery. These formulas use data points collected during biometry, primarily axial length, corneal curvature, and anterior chamber depth, to estimate where the new lens will sit inside the eye and what optical power it needs.
Several formula generations exist:
- First- and second-generation formulas relied on linear regression from large datasets of surgical outcomes.
- Third-generation formulas, such as SRK/T, Hoffer Q, and Holladay, introduced theoretical optical models that built upon linear regression, improving accuracy across a wider range of eye sizes.
- Newer-generation formulas incorporate additional variables, including lens thickness and corneal diameter, to refine predictions further.
No single formula performs best for every eye. Surgeons often run multiple formulas and compare results, selecting the one most suited to a patient’s specific anatomy. This multi-formula approach is one of the most practical ways to catch outlier predictions before they reach the operating room.
How Do Modern Formulas Differ From Older Ones?
Modern formulas differ from older ones by using larger datasets, more anatomical variables, and artificial intelligence to improve predictive accuracy. Earlier third-generation formulas like SRK/T and Hoffer Q rely on a limited set of measurements and fixed theoretical assumptions about lens position. While effective for average-length eyes, their accuracy decreases in unusual anatomies.
According to a study published through Kansas City University’s DigitalCommons, modern AI-based formulas like Hill-RBF 3.0 achieved comparable or superior predictive accuracy over traditional and other AI-based formulas, enhancing clinical outcomes. Formulas such as Olsen also use ray-tracing, capturing optical behavior that simpler models approximate.
For patients with very long or very short eyes, this generational leap matters most. Older formulas tend to over- or under-correct in these cases, while newer formulas handle anatomical extremes with greater consistency. As formula technology continues advancing, the gap between predicted and actual refractive outcomes narrows, though biological variability still prevents perfection.
With IOL power selected, understanding why biometry still falls short of perfect precision helps set realistic expectations before surgery. Beyond precise measurements, understanding that modern cataract surgery is pain-free and safe helps alleviate common patient concerns before the procedure.
Why Is Biometry Not Perfectly Exact?
Biometry is not perfectly exact because living eyes introduce biological variability, surface irregularities, and measurement tolerances that no instrument can fully eliminate. The following subsections explain how these factors limit precision.
How Do Biological Variations Limit Measurement Precision?
Biological variations limit measurement precision because no two eyes share identical internal dimensions, and those dimensions shift over time. Axial length, anterior chamber depth, and lens thickness all vary naturally between individuals and even between a patient’s own left and right eyes. Age-related lens growth, for instance, gradually changes the eye’s internal geometry in ways that differ from person to person.
These subtle anatomical differences mean that population-based averages embedded in IOL calculation formulas cannot perfectly represent every individual eye. Even when instruments capture highly repeatable readings, the underlying biology introduces a margin of uncertainty that technology alone cannot resolve.
How Does Tear Film Quality Affect Biometry Readings?
Tear film quality affects biometry readings because the tear layer is the first optical surface that light-based instruments must pass through. When this layer is unstable, uneven, or too thin, the corneal surface data captured during keratometry and axial length measurement becomes less consistent.
According to a study published on ResearchGate, tear film instability and corneal surface irregularity are important sources of variability in keratometric and axial length measurements in patients with cataracts. Even artificial tears can temporarily alter readings; research published in PMC (2024) found that artificial tears significantly affect axial length and central corneal thickness measurements, recommending clinicians wait at least five minutes after installation before taking biometry. For patients with dry eye disease, this variability can compound across repeated measurements, making consistent data harder to obtain.
Why Can Small Measurement Errors Cause Significant Refractive Surprises?
Small measurement errors can cause significant refractive surprises because the eye’s optical system is extremely sensitive to dimensional changes. A difference of just 0.35 to 0.40mm in axial length translates to roughly 1 diopters of refractive error in adults, which is enough to shift a patient’s postoperative outcome from the intended target.
A refractive surprise occurs when the postoperative refractive outcome differs significantly from the intended target after cataract surgery. Because IOL power calculations rely on multiple measured variables, small inaccuracies in corneal curvature, anterior chamber depth, or axial length can compound through the formula, amplifying the final prediction error. This cascading effect is why even highly precise instruments cannot guarantee a perfect refractive result in every case.
How Does Corneal Shape Irregularity Affect Accuracy?
Corneal shape irregularity affects accuracy because standard keratometry assumes the cornea is a smooth, symmetrical surface. When astigmatism is irregular, or the cornea has been reshaped by prior surgery, scarring, or conditions like keratoconus, the measured curvature values may not represent the eye’s true refractive power.
Irregular corneas scatter light in unpredictable patterns, making it difficult for optical biometers to obtain clean, repeatable readings. IOL calculation formulas then receive corneal data that does not reflect the actual optics of the eye. This mismatch between measured and functional corneal shape is one of the most common reasons biometry predictions fall outside acceptable accuracy ranges in complex cases.
Why Is Biometry Less Predictable in Very Long or Short Eyes?
Biometry is less predictable in very long or short eyes because IOL calculation formulas were historically optimized for average-length eyes, typically between 22.5 and 24.2 mm. Eyes outside this range magnify the effect of even minor measurement errors on the final refractive outcome.
According to a study published in International Ophthalmology (Springer, 2022), new-generation formulas such as Barrett Universal II and Olsen achieved higher percentages of accuracy than SRK/T, Hoffer Q, and Holladay I in axial myopic eyes. Despite these improvements, extreme axial lengths remain the most challenging cases for refractive prediction. Very short eyes have proportionally stronger IOL powers, where small calculation shifts produce larger diopter swings, while very long eyes are prone to greater measurement variability in the posterior segment.
Understanding these inherent limitations helps set realistic expectations for what cataract surgery can achieve.
What Is a Refractive Surprise After Cataract Surgery?
A refractive surprise is an unexpected difference between the intended vision target and the actual postoperative outcome after cataract surgery. The sections below cover how often this occurs and what options exist when the result falls outside expectations.
How Common Are Refractive Surprises?
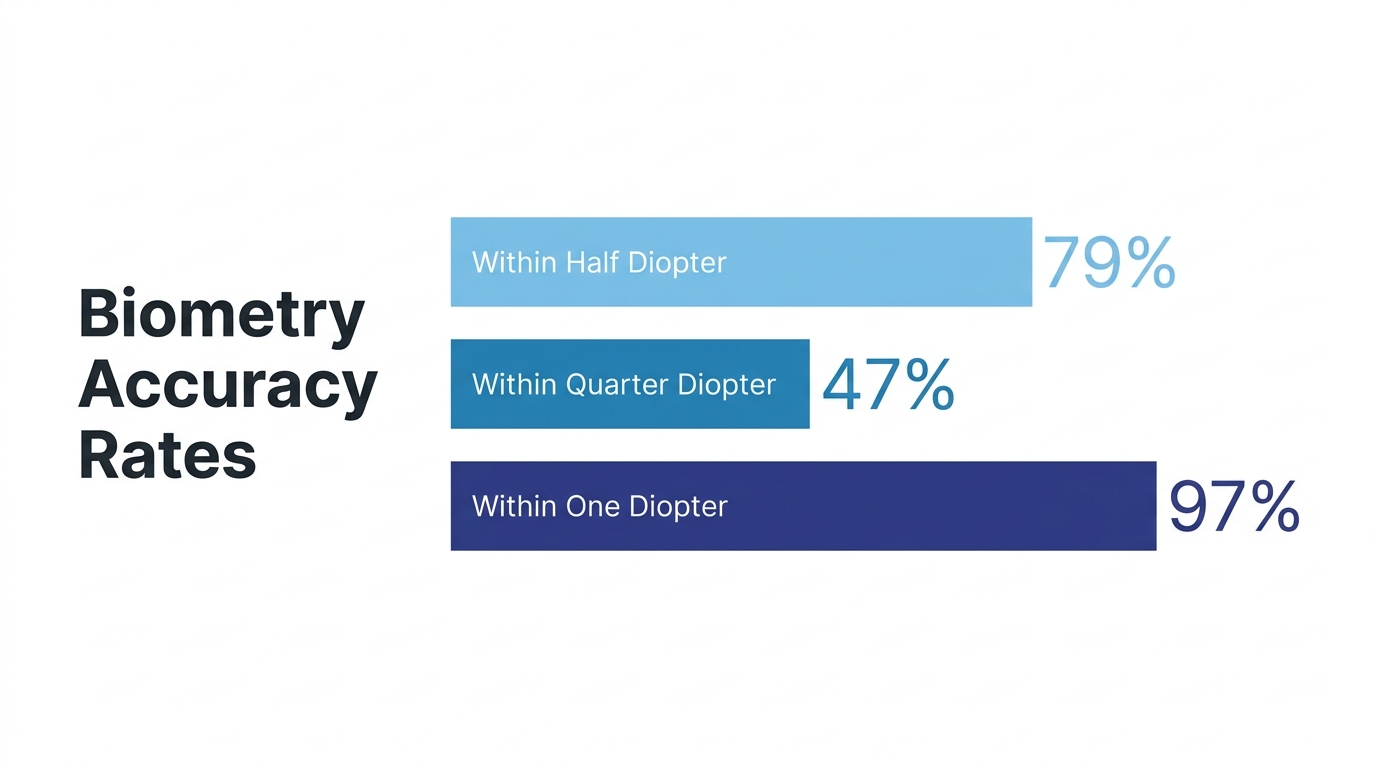
Refractive surprises are relatively uncommon when modern biometry and IOL formulas are used, though they are not rare enough to dismiss. According to the American Academy of Ophthalmology, approximately 79% of eyes achieve outcomes within 0.5 D of the target, 47% land within 0.25 D, and 97% fall within 1.0 D in standard cataract surgery. That means roughly 1 in 5 eyes finishes outside the tightest accuracy window, and about 3 in 100 experience a clinically meaningful miss beyond 1.0 D.
External confounding factors, such as patient age and previous refractive state, can influence these benchmarks. For patients with prior corneal refractive surgery or unusual eye anatomy, the likelihood of a refractive surprise increases. Even small biometry measurement variations, when compounded through IOL power calculation formulas, can shift the final outcome enough to notice. Given these potential outcomes, patients should discuss the possibility of needing glasses post-surgery with their ophthalmologist, and consider preparing for possible glasses use.
What Can Be Done If the Outcome Doesn’t Match the Target?
What can be done if the outcome doesn’t match the target depends on the size and nature of the refractive error. Options may include:
- Updated spectacle or contact lens prescription to correct a minor residual refractive error.
- Laser enhancement procedures, such as LASIK or PRK, to fine-tune corneal curvature after healing stabilizes.
- IOL exchange or secondary piggyback lens implantation for larger refractive misses where a lens power adjustment is needed.
Specialized formulas can also help prevent surprises before they happen. The Barrett True-K formula achieved the highest proportion of eyes within 0.50 D (71.9%) in patients with prior refractive surgery, according to a review published by EyeWorld (ASCRS). For most patients, the key is open communication with the surgeon before and after surgery, so expectations align with what biometry can realistically predict.
Understanding refractive surprises helps frame why prior refractive procedures like LASIK or PRK add complexity to biometry accuracy.
How Does Prior LASIK or PRK Affect Biometry Accuracy?
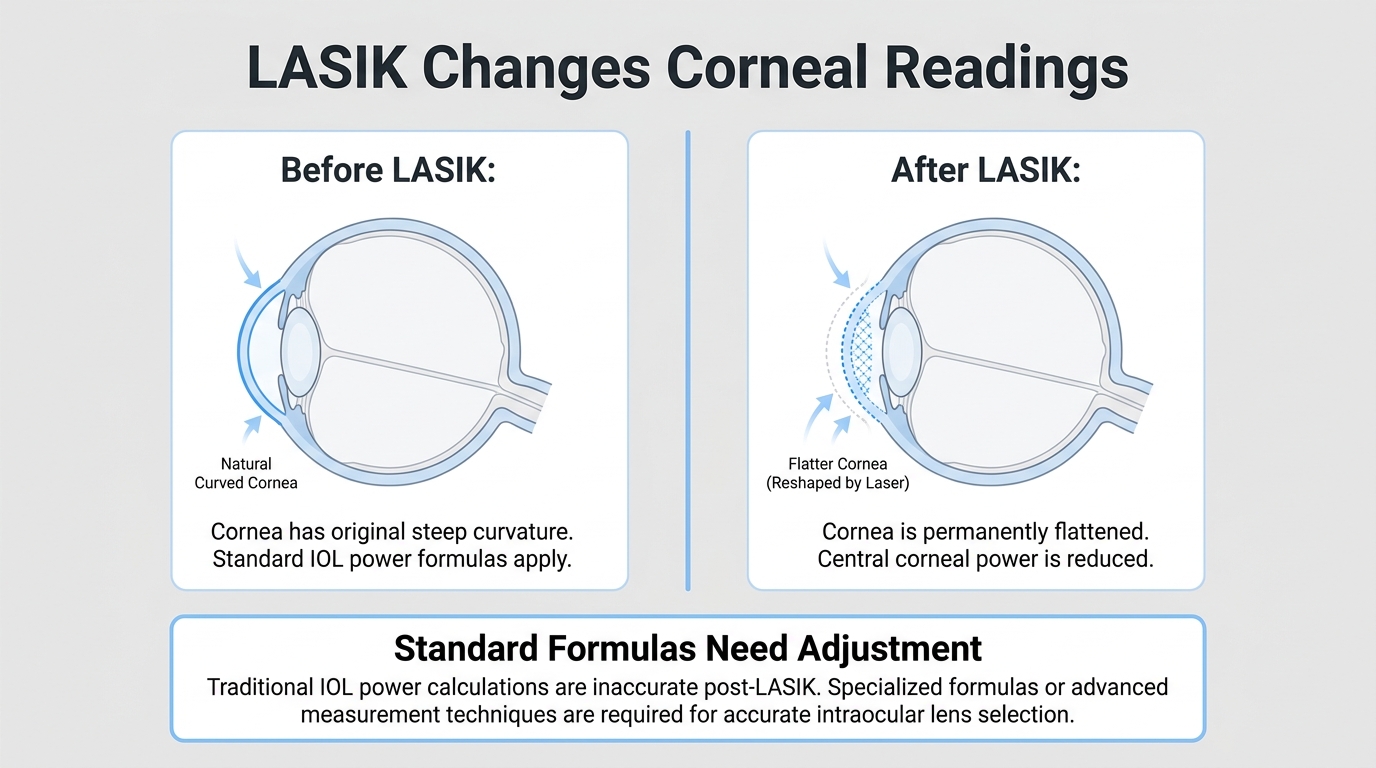
Prior LASIK or PRK affects biometry accuracy by altering the cornea’s natural curvature, which causes standard keratometry readings to overestimate corneal power and leads to IOL calculation errors. Specialized formulas and intraoperative tools help surgeons compensate for these changes.
Refractive surgery reshapes the anterior corneal surface to correct myopia, hyperopia, or astigmatism. Standard biometry devices measure the front corneal curvature and apply a fixed ratio to estimate total corneal power, assuming a natural relationship between the front and back surfaces. After LASIK or PRK, that assumed ratio no longer holds because only the anterior surface was modified. This mismatch can produce keratometry values that do not reflect the cornea’s true refractive power, often resulting in a hyperopic surprise if a standard IOL formula is used without correction.
The effective lens position prediction also suffers. Many IOL formulas use corneal curvature as an input to estimate where the implant will sit inside the eye. A flatter post-refractive cornea may cause the formula to predict a more anterior lens position than what actually occurs, compounding the power calculation error.
To address these challenges, surgeons rely on formulas specifically designed for post-refractive eyes. According to a review published by EyeWorld (ASCRS), the Barrett True-K formula achieved the highest proportion of eyes within 0.50 D of target refraction at 71.9% among post-refractive surgery patients. Intraoperative wavefront aberrometry can further refine lens selection by measuring the eye’s optical system in real time during surgery, which is particularly valuable when preoperative corneal data may be unreliable.
Having pre-LASIK or pre-PRK records, including original keratometry values and the surgical correction amount, significantly improves calculation accuracy. When those records are unavailable, clinical history methods and online calculators, such as the ASCRS post-refractive IOL calculator, offer alternative pathways. Patients who have undergone prior refractive surgery should always inform their cataract surgeon so the appropriate adjustments can be made before IOL selection.
With post-refractive considerations addressed, the next section explores which biometry technologies surgeons use today.
Which Biometry Technologies Are Used Today?
The biometry technologies used today include optical biometry, contact ultrasound A-scan, and immersion ultrasound. Each method measures eye dimensions differently, with distinct advantages depending on the clinical situation.
How Does Optical Biometry Work?
Optical biometry works by using infrared light to measure the anatomical characteristics of the eye without touching the corneal surface. The device directs a beam of light into the eye and calculates distances based on reflected signals, capturing axial length, corneal curvature, and anterior chamber depth in a single automated session.
According to ZEISS Medical Technology, optical biometry is a highly accurate, non-invasive, automated method for measuring the anatomical characteristics of the eye. Because this technique relies on light wavelengths rather than sound, it captures finer detail and incorporates the actual thickness of the retina into its calculations. The result is a precise axial length measurement that does not require corneal contact, reducing both patient discomfort and operator-dependent variability. For most cataract surgery candidates, optical biometry represents the preferred first-line measurement approach.
How Does Ultrasound A-Scan Biometry Work?
Ultrasound A-scan biometry works by emitting a high-frequency sound wave through a probe placed directly on the cornea. The sound pulse travels through the eye’s internal structures, and the device calculates distances based on echo return times from each tissue boundary.
This contact method remains valuable when optical biometry cannot obtain a reading, such as in eyes with dense cataracts or significant media opacities that block light transmission. However, because the probe physically touches the cornea, slight compression of the corneal surface can shorten the measured axial length. That compression introduces a small but clinically meaningful source of error, which is why careful technique and consistent probe pressure are essential during contact A-scan measurements.
When Is Immersion Ultrasound Preferred Over Optical Methods?
Immersion ultrasound is preferred over optical methods when dense cataracts or corneal opacities prevent reliable light-based readings, and when eliminating corneal compression error is clinically important.
During immersion biometry, a saline-filled shell sits over the eye, and the ultrasound probe is suspended in the fluid without touching the cornea. As the American Academy of Ophthalmology’s EyeWiki notes, axial length is defined as the distance from the anterior corneal surface to the retinal pigment epithelium, and this measurement can be obtained using optical or ultrasound (contact or immersion) methods. Because the immersion technique avoids direct corneal contact, it produces longer and more accurate axial length readings than contact A-scan. In clinical practice, immersion ultrasound serves as a reliable fallback that bridges the gap between contact methods and optical biometry.
With measurement technologies established, practical strategies for improving biometry accuracy become the next consideration.
What Can Surgeons Do to Improve Biometry Accuracy?
Surgeons can improve biometry accuracy by taking multiple measurements and using real-time intraoperative verification tools. The following subsections cover repeated measurement protocols and intraoperative aberrometry.
How Do Multiple Measurements Help Reduce Error?
Multiple measurements help reduce error by averaging out the small variabilities inherent in each individual reading. Biometric values for axial length, keratometry, and anterior chamber depth can fluctuate slightly between captures due to tear film changes, patient fixation shifts, and instrument noise.
When a surgeon captures several readings and compares them for consistency, outlier measurements become easy to identify and discard. The averaged result from concordant readings produces a more reliable input for IOL power calculation formulas. Most experienced surgeons take at least three to five measurements per parameter and confirm that the standard deviation falls within acceptable limits before proceeding with lens selection. In practice, this straightforward step is one of the most underappreciated safeguards against refractive surprises, particularly in eyes with borderline signal quality or irregular corneal surfaces.
How Does Intraoperative Aberrometry Refine IOL Selection?
Intraoperative aberrometry refines IOL selection by measuring the eye’s refractive state in real time during surgery, after the natural lens has been removed. This allows the surgeon to verify or adjust the preoperatively chosen IOL power before the procedure is complete.
Systems like the ORA (Optiwave Refractive Analysis) capture wavefront data from the aphakic eye and recommend an IOL power based on live measurements rather than preoperative estimates alone. According to a study published in the Journal of Cataract & Refractive Surgery, preoperative Barrett Universal II calculations placed 77% of eyes within 0.50 D of target, compared to 57% for non-optimized intraoperative aberrometry, highlighting that aberrometry performs best when its readings are optimized with surgeon-adjusted nomograms. The technology can also effectively predict refractive outcomes in eyes receiving toric IOLs, where rotational alignment precision is critical.
For patients with prior corneal refractive surgery or unusual anatomy, intraoperative aberrometry provides an invaluable second check that preoperative data alone cannot offer. The primary method for removing the cataract during the procedure itself is often phacoemulsification, a technique leveraging ultrasonic energy for precise lens removal. With these surgical strategies established, informed patient expectations complete the preparation process.
What Should Patients Understand Before Cataract Surgery?
Patients should understand that biometry provides highly accurate measurements, but no measurement system delivers perfection. The following subsections cover how education prepares you for IOL decisions and the key takeaways about biometry’s inherent limitations.
How Can Education Help You Prepare for IOL Decisions?
Education can help you prepare for IOL decisions by setting realistic expectations about what biometry can and cannot guarantee. When a guide explains how measurements like axial length, corneal curvature, and anterior chamber depth feed into IOL power calculations, patients gain the context needed to understand why a specific lens is recommended and why outcomes may vary slightly from the target refraction.
Informed patients are better equipped to weigh trade-offs between IOL options, such as monofocal, multifocal, or toric lenses. Preoperative conversations should cover factors that can influence accuracy, including tear film quality, prior refractive surgery, and unusual eye anatomy. This transparency reduces anxiety if a minor refractive surprise occurs and helps patients participate meaningfully in shared decision-making with their ophthalmologist. For most patients, understanding the process matters more than memorizing technical details. During these discussions, patients can also learn about different surgical approaches, such as laser cataract surgery, and their potential impact on visual outcomes.
What Are the Key Takeaways About Biometry and Its Limitations?
The key takeaways about biometry and its limitations center on three points: biometry is essential, highly accurate, yet inherently imperfect. According to the American Academy of Ophthalmology, approximately 79% of eyes achieve outcomes within 0.5 diopters of target values, and 97% fall within 1.0 diopter in standard cataract surgery.
Core points to remember:
- Biometry measures axial length, corneal curvature, anterior chamber depth, and lens thickness to calculate IOL power.
- Biological variability, tear film instability, and corneal irregularities can introduce small measurement errors that affect final refraction.
- Modern formulas like Barrett Universal II and Hill-RBF 3.0 improve predictive accuracy, but no formula eliminates uncertainty entirely.
- Eyes with prior LASIK or PRK, or those with very long or short axial lengths, carry higher risk of refractive surprise.
- Surgeons use strategies such as repeated measurements and intraoperative aberrometry to minimize error.
Biometry remains one of the most reliable diagnostic tools in ophthalmology. When patients understand both its precision and its boundaries, they approach cataract surgery with confidence grounded in realistic expectations. Eye Surgery Today provides resources to help patients navigate these decisions with clarity.
