An intraocular lens (IOL) is a small, artificial lens implanted inside the eye to replace the natural crystalline lens removed during cataract surgery, restoring the eye’s ability to focus light onto the retina. Without this replacement, the eye lacks the refractive power needed for functional vision.
This guide covers IOL types and how they work, vision goals and candidacy factors, preoperative measurements, potential benefits and risks of premium lenses, and cost and insurance considerations.
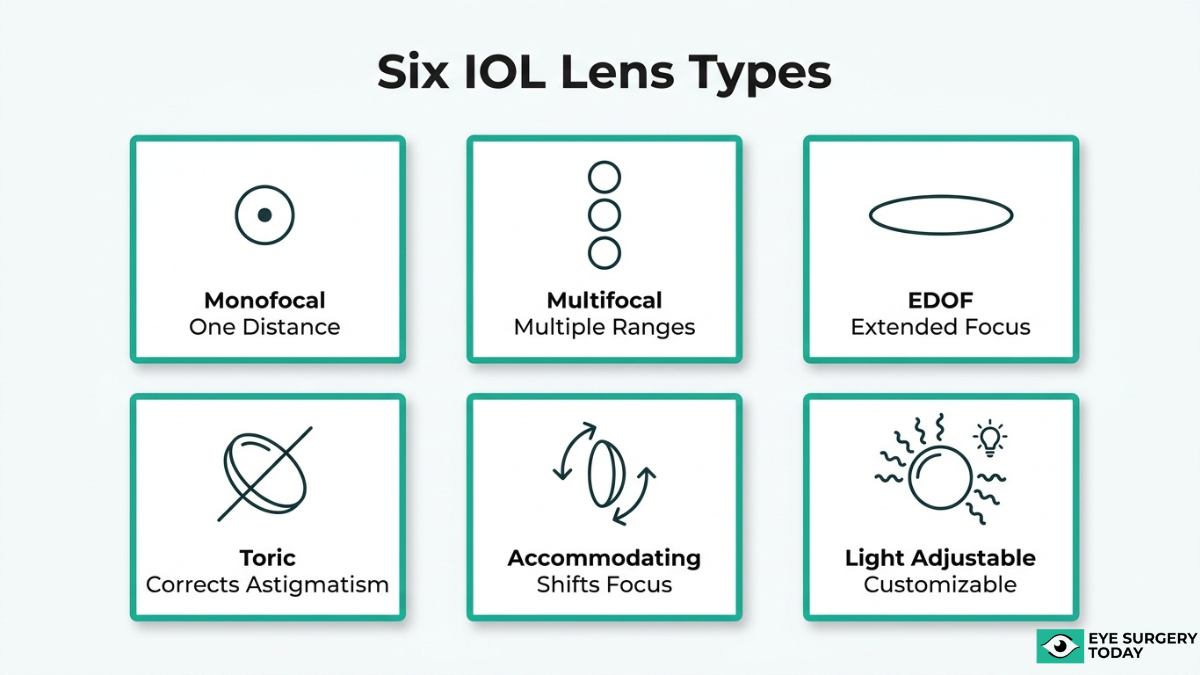
Modern IOLs range from monofocal lenses that optimize clarity at a single distance to premium options such as multifocal, extended depth of focus, toric, accommodating, and light adjustable designs. Each category addresses different visual needs through distinct optical mechanisms.
Candidacy for premium IOLs depends on ocular health, lifestyle priorities, and realistic expectations. Pre-existing conditions such as glaucoma, macular degeneration, corneal irregularities, and diabetic retinopathy may limit which lenses can deliver reliable results. Patients with healthy retinas and stable corneal measurements tend to be the strongest candidates for advanced designs.
Accurate preoperative testing, including ocular biometry, corneal topography, and retinal imaging, forms the foundation of lens selection. These measurements feed into IOL power calculation formulas that determine the correct lens strength for each eye.
Premium IOLs may reduce dependence on glasses and correct astigmatism, yet they can also introduce visual disturbances such as halos and glare. Neuroadaptation plays a role in long-term satisfaction, and outcomes vary by patient.
Cost is a practical factor as well. Standard monofocal lenses are generally covered by Medicare, while premium upgrades carry additional out-of-pocket expenses that patients should plan for before surgery.
What Is an Intraocular Lens and Why Is It Needed After Cataract Surgery?
An intraocular lens (IOL) is a small, artificial lens implanted inside the eye to replace the natural crystalline lens after cataract surgery. During the procedure, the clouded natural lens is removed, and the IOL restores the eye’s ability to focus light onto the retina. Without this replacement, the eye would lack the refractive power needed for functional vision.
The natural crystalline lens plays a central role in bending light to form clear images. When cataracts cause this lens to become opaque, vision gradually deteriorates. Because the entire lens is removed during cataract surgery, an IOL is needed to take over that optical function. Modern IOLs are biocompatible, designed to remain stable inside the eye for a lifetime, and available in several designs that address different visual needs.
Choosing the right IOL is one of the most consequential decisions in the cataract surgery process. The sections below cover the major lens types, candidacy factors, vision goals, potential risks, and cost considerations that can help guide that choice.
What Are the Types of Intraocular Lenses Available After Cataract Surgery?
The types of intraocular lenses available after cataract surgery include monofocal, multifocal, extended depth of focus, toric, accommodating, and light adjustable lenses. Each IOL type addresses different visual needs.
Monofocal IOLs
Monofocal IOLs are intraocular lenses designed to provide the best possible vision at one distance. Most patients choose a monofocal lens set for clear distance vision, then use reading glasses for near tasks. Because monofocal IOLs focus light on a single focal point, they typically produce fewer visual disturbances such as halos or glare compared to premium alternatives. This simplicity makes them the most commonly implanted IOL worldwide and the standard lens covered by insurance. For patients whose primary goal is reliable distance clarity without added cost, a monofocal IOL remains an excellent choice.
Multifocal IOLs
Multifocal IOLs are intraocular lenses that split incoming light into multiple focal points, providing vision at near, intermediate, and distance ranges. According to Cataract & Refractive Surgery Today Europe, multifocal IOLs feature either refractive or diffractive optics, varying in how light is distributed and centered on the retina. Trifocal designs, a subset of multifocal lenses, have demonstrated stronger near vision performance than hybrid multifocal-EDOF combinations in meta-analysis data, while both categories achieved high patient satisfaction. The tradeoff is worth noting: because light is divided among focal zones, some patients notice halos or glare, particularly in low-light conditions. Patients who strongly prefer reducing glasses dependence across all distances often find multifocal IOLs well suited to that goal.
Extended Depth of Focus IOLs
Extended depth of focus (EDOF) IOLs are intraocular lenses that elongate a single focal point rather than splitting light into multiple zones. This design may provide a continuous range of vision from distance to intermediate. According to a 2024 publication in the Journal of Cataract & Refractive Surgery, measurable ANSI/AAO criteria now differentiate EDOF lenses from standard monofocal IOLs based on their extended range. Because EDOF IOLs avoid the sharp light-splitting of multifocal designs, they tend to produce fewer photic disturbances. However, near vision at very close range may still require reading glasses. For patients who prioritize functional intermediate vision with a lower risk of halos, EDOF lenses represent a practical middle ground.
Toric IOLs
Toric IOLs are intraocular lenses specifically engineered to correct pre-existing corneal astigmatism during cataract surgery. Astigmatism causes an irregularly shaped cornea that bends light unevenly, resulting in blurred or distorted vision at all distances. A toric lens has different optical powers along its meridians, counteracting that uneven curvature. Precise rotational alignment during implantation is critical; even small degrees of misalignment can reduce the astigmatism correction. Toric IOLs can be combined with other technologies, such as multifocal or EDOF optics, for patients who want both astigmatism correction and a broader range of focus. For anyone with significant astigmatism, a toric IOL is often the most effective path to clear uncorrected distance vision.
Accommodating IOLs
Accommodating IOLs are intraocular lenses designed to allow both good distance vision and near vision. According to a review published in the National Institutes of Health (PMC), this dual capability is achieved through the contraction and relaxation of ciliary muscles, which shift the lens position inside the eye. Unlike multifocal IOLs that split light, accommodating lenses attempt to mimic the eye’s natural focusing mechanism. The range of near focus they deliver can be more modest than what multifocal designs provide, so some patients still need reading glasses for fine print. Ongoing research continues to refine accommodating IOL designs, and newer models aim to expand the achievable range of clear near vision.
Light Adjustable Lenses
Light adjustable lenses are intraocular lenses whose optical power can be fine-tuned after cataract surgery using ultraviolet light. According to U.S. FDA documentation, the Light Adjustable Lens (LAL) is a posterior chamber, UV-absorbing, three-piece, foldable, photoreactive silicone IOL adjusted with low levels of ultraviolet light. This post-surgical customization allows the surgeon to optimize the prescription once the eye has healed, reducing residual refractive error. Patients receiving a LAL must wear special UV-protective glasses between treatments to prevent unintended power changes. The LAL is contraindicated in patients taking systemic medications that may increase UV sensitivity, such as tetracycline, doxycycline, and psoralens. For patients who value precision and are willing to complete the adjustment protocol, the LAL offers a level of post-operative refinement unavailable with fixed-power lenses.
With these lens categories in mind, understanding how monofocal and premium IOLs compare can further clarify the right choice.
How Does a Monofocal IOL Differ From a Premium IOL?
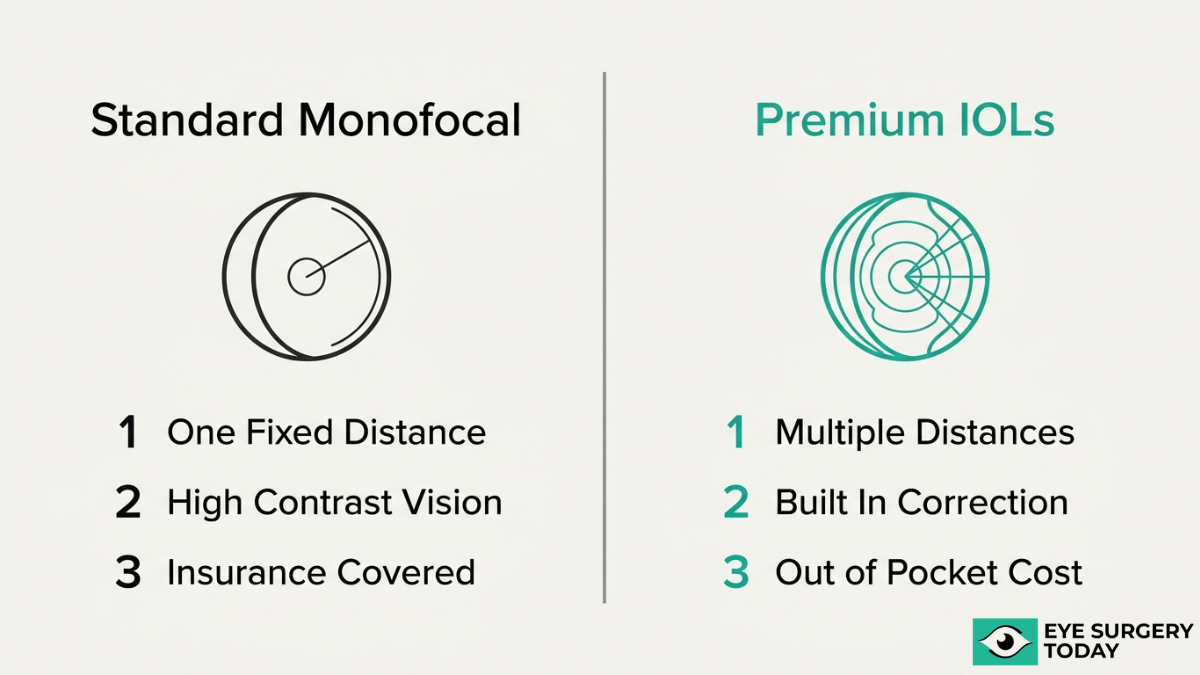
A monofocal IOL differs from a premium IOL primarily in the range of vision each lens provides. Monofocal lenses optimize sight at a single focal point, while premium IOLs use advanced optics to address multiple distances or correct specific refractive errors. The differences span optical design, visual outcomes, cost structure, and candidacy requirements.
A monofocal IOL uses a single-focus optical design to deliver sharp vision at one predetermined distance, typically far. According to the American Academy of Ophthalmology, monofocal lenses are designed to provide the best possible vision at one distance. Most patients who choose a monofocal lens still rely on reading glasses or progressives for near and intermediate tasks. Because the optic splits no light between focal zones, monofocal lenses produce high contrast sensitivity and minimal photic phenomena, such as halos or glare. Insurance, including Medicare, generally covers monofocal IOLs as the standard of care.
Premium IOLs encompass several categories, each engineered to expand functional vision beyond a single focal point:
- Multifocal IOLs use refractive or diffractive ring patterns to distribute light across two or three focal zones, reducing dependence on glasses for near, intermediate, and distance tasks.
- Extended depth of focus (EDOF) IOLs elongate a single focal point to create a continuous range from distance through intermediate vision, with fewer visual disturbances than traditional multifocals.
- Toric IOLs incorporate cylinder correction into the lens optic to neutralize pre-existing corneal astigmatism, improving uncorrected distance acuity.
- Accommodating IOLs shift position within the eye using ciliary muscle contraction, mimicking the natural lens’s ability to change focus.
- Light Adjustable Lenses allow postoperative power customization through UV light treatments, enabling fine-tuned refractive outcomes after the eye has healed.
The trade-offs between these two categories matter in practice. Premium IOLs offer greater spectacle independence, yet they may introduce photic phenomena; halos and glare tend to be more pronounced with presbyopia-correcting designs than with monofocal lenses. Premium options also carry additional out-of-pocket costs because Medicare does not cover the upgrade portion of presbyopia-correcting or astigmatism-correcting IOLs. Not every patient qualifies for a premium design either, since conditions such as moderate to severe glaucoma or certain retinal diseases can be contraindications.
For many patients, the deciding factor comes down to how much they value reduced glasses dependence versus optical simplicity, balanced against budget and ocular health. Understanding these core differences is the first step toward identifying which vision goals matter most to you.
What Vision Goals Should You Consider Before Choosing a Lens?
The vision goals you should consider before choosing a lens include distance clarity, glasses independence, astigmatism correction, and near vision for detail work. Each priority aligns with different IOL types.

What If Your Priority Is Clear Distance Vision?
If your priority is clear distance vision, a monofocal IOL set for distance is typically the most straightforward option. According to the American Academy of Ophthalmology, monofocal lenses are designed to provide the best possible vision at one distance. When set for far focus, these lenses can deliver sharp clarity for activities such as driving, watching television, and recognizing faces across a room.
The trade-off is predictable: reading glasses will likely still be needed for close tasks. For patients who value reliable, high-contrast distance vision above all else, monofocal lenses remain a proven choice with decades of clinical success behind them.
What If Your Priority Is Reducing Dependence on Glasses?
If your priority is reducing dependence on glasses, multifocal or extended depth of focus IOLs may help address multiple focal points within a single lens. These premium options split or elongate the focal range so that both distance and intermediate, or even near, tasks can be performed without corrective eyewear.
Candidates who are most likely to benefit include those who:
- Dislike switching between reading glasses and distance glasses throughout the day.
- Spend significant time on intermediate-distance tasks, such as computer work or cooking.
- Have healthy retinas and no significant corneal irregularities.
Complete glasses independence is not guaranteed for every patient. Some individuals may still prefer light reading glasses for prolonged fine print. Discussing realistic expectations with a surgeon helps set appropriate goals before committing to a premium lens. Ultimately, a deep understanding of lifestyle preferences helps guide the choice toward an IOL that best supports daily activities and personal vision needs.
What If Your Priority Is Correcting Astigmatism?
If your priority is correcting astigmatism, a toric IOL is specifically engineered to neutralize the uneven corneal curvature that causes blurred or distorted vision. Toric lenses correct pre-existing corneal astigmatism at the time of cataract removal, addressing two problems in a single procedure.
Key considerations for astigmatism correction include:
- The degree of corneal astigmatism, typically measured during preoperative biometry.
- Precise rotational alignment of the toric lens during implantation, since even small misalignments can reduce effectiveness.
- Whether combining astigmatism correction with multifocal or EDOF optics suits the patient’s broader visual needs.
Patients with significant astigmatism who skip toric correction often remain dependent on glasses for distance vision, which can undermine the benefits of cataract surgery itself.
What If You Need Strong Near Vision for Detail Work?
If you need strong near vision for detail work, multifocal IOLs with a dedicated near-focus zone or accommodating IOLs may help provide the close-range clarity required for tasks such as reading, sewing, or working with small instruments. These lens designs prioritize functional near vision alongside distance correction.
It is worth noting that Medicare does not cover the additional costs of presbyopia-correcting IOLs, as outlined by the Centers for Medicare and Medicaid Services. This means patients who choose a near-vision-optimized premium lens will typically pay out of pocket for the upgrade beyond a standard monofocal IOL.
For those whose daily routines demand sustained close focus, investing in a lens that supports strong near acuity can meaningfully improve quality of life. With lens selection aligned to specific vision goals, the next step is understanding which clinical factors determine candidacy for premium IOL options.
Who Is a Good Candidate for Multifocal or Extended Depth of Focus IOLs?
A good candidate for multifocal or extended depth of focus IOLs is typically someone with healthy eyes, realistic expectations, and a strong desire to reduce dependence on glasses after cataract surgery. Candidacy depends on ocular health, lifestyle needs, and willingness to adapt to new visual characteristics.
Patients who may benefit most from these premium lenses generally share several key traits:
- Healthy retinas and corneas. Conditions such as macular degeneration, significant corneal scarring, or irregular astigmatism can compromise the optical performance of multifocal and EDOF designs.
- No moderate to severe glaucoma. Advanced glaucoma limits the visual field and contrast sensitivity that these lenses rely on for optimal function.
- Strong motivation to reduce glasses use. Multifocal IOLs split light across multiple focal points, while EDOF IOLs elongate a single focal point to extend the range of clear vision from distance through intermediate.
- Tolerance for visual trade-offs. Photic phenomena, such as halos and glare, can be more noticeable with presbyopia-correcting lenses. Candidates should understand this possibility before proceeding.
- Active lifestyles with varied visual demands. Those who frequently shift between distance, intermediate, and near tasks without wanting to reach for reading glasses often find the greatest value in these designs.
- Realistic expectations about near vision. According to a 2022 study published in Scientific Reports, patients implanted with EDOF IOLs achieved high satisfaction levels, although they may experience significantly worse near vision compared to multifocal groups.
Personality and adaptability also matter. Neuroadaptation, the brain’s process of adjusting to a new optical system, plays a meaningful role in long-term satisfaction. Patients who are flexible and patient during the weeks following surgery tend to report better outcomes than those expecting instant perfection.
The decision between a multifocal and an EDOF lens often comes down to prioritizing either a broader range of sharp focal points or smoother intermediate vision with fewer visual disturbances. Neither design suits every patient equally, which is why a thorough preoperative evaluation is essential. Understanding who may not qualify for premium IOLs is equally important for setting appropriate expectations.
Who May Not Be a Good Candidate for Premium IOLs?
Not everyone is a good candidate for premium IOLs. Certain pre-existing eye conditions can limit how well these lenses perform, potentially reducing visual quality or increasing dissatisfaction. The sections below cover macular degeneration, glaucoma, corneal irregularities, and diabetic retinopathy.
Why Might Macular Degeneration Affect Premium IOL Candidacy?
Macular degeneration may affect premium IOL candidacy because this condition damages the central retina, which is essential for the sharp, detailed vision that premium lenses are designed to optimize. Multifocal and extended depth of focus IOLs split incoming light across multiple focal points, and this light-splitting design relies on a healthy macula to process the resulting image clearly. When macular function is compromised, the brain may struggle to interpret the divided light, leading to reduced contrast sensitivity and blurred central vision regardless of lens quality. For patients with even early-stage macular degeneration, a monofocal IOL often provides a more predictable visual outcome. A thorough retinal evaluation before surgery helps your ophthalmologist determine whether a premium lens can deliver meaningful benefit.
Why Might Glaucoma Affect Premium IOL Candidacy?
Glaucoma may affect premium IOL candidacy because this disease progressively damages the optic nerve, narrowing the visual field and reducing contrast sensitivity. Premium IOLs, particularly multifocal designs, distribute light across several focal zones. This distribution can worsen contrast loss in eyes already compromised by glaucomatous damage. According to the Journal of Current Glaucoma Practice, premium IOLs are contraindicated in patients with moderate to severe glaucoma, and extreme caution is advocated for patients with ocular hypertension. Even mild glaucoma warrants careful consideration, since visual field deficits can make the photic phenomena associated with premium lenses more noticeable and disruptive. In clinical practice, a monofocal IOL paired with reading glasses is frequently the safer, more satisfying choice for patients managing glaucoma.
Why Might Corneal Irregularities Affect Premium IOL Candidacy?
Corneal irregularities may affect premium IOL candidacy because the cornea is the eye’s primary refracting surface, and its shape directly influences how light reaches the implanted lens. Conditions such as keratoconus, corneal scarring, and significant irregular astigmatism distort the incoming light wavefront in unpredictable ways. Premium IOLs, especially multifocal and EDOF designs, rely on a smooth, regular corneal surface to focus light precisely across their optical zones. When that surface is uneven, the lens cannot distribute light as intended, often producing ghosting, glare, or blurred images that undermine the lens’s intended benefit. Accurate preoperative corneal topography helps identify these irregularities before lens selection.
Why Might Diabetic Retinopathy Affect Premium IOL Candidacy?
Diabetic retinopathy may affect premium IOL candidacy because this condition causes progressive damage to retinal blood vessels, leading to swelling, leakage, and potential vision loss that fluctuates over time. Premium IOLs perform best when the retina can consistently process the complex light patterns these lenses produce. Diabetic macular edema, a common complication, directly impairs central vision and can worsen after cataract surgery. Because retinopathy can progress unpredictably, the long-term visual gains of a premium IOL become difficult to guarantee. Patients with active or poorly controlled diabetic retinopathy are generally advised toward monofocal lenses, which offer more stable, forgiving visual outcomes. Stabilizing blood sugar and managing retinal health before surgery gives your ophthalmologist clearer insight into which lens may deliver lasting results.
Who Is a Good Candidate for Toric IOLs?
A good candidate for toric IOLs is a cataract patient with pre-existing corneal astigmatism who wants to reduce dependence on glasses for distance vision after surgery. Candidacy depends on the amount and regularity of astigmatism, overall eye health, and realistic visual expectations.
Toric IOLs correct astigmatism by compensating for the uneven curvature of the cornea, which causes light to focus at multiple points rather than a single focal point. Patients with regular corneal astigmatism of 1.0 diopter or greater typically benefit most from this correction. Those with lower amounts may still be candidates, though the visual improvement over a standard monofocal lens becomes less pronounced.
Stable corneal measurements are essential. Conditions that cause irregular or fluctuating astigmatism, such as keratoconus or significant corneal scarring, may disqualify a patient because the toric lens relies on precise alignment with the corneal meridians. According to a clinical assessment published in Ophthalmology (Journal of the American Academy of Ophthalmology), toric IOLs are effective at correcting pre-existing corneal astigmatism and providing good uncorrected distance visual acuity, with all major platforms performing well.
Ideal candidates also meet several additional criteria:
- Healthy retinas free of conditions that could limit visual outcomes, such as macular degeneration or advanced diabetic retinopathy.
- No moderate to severe dry eye disease, which can distort corneal topography readings and compromise lens calculations.
- Willingness to understand that toric IOLs primarily optimize distance vision; reading glasses may still be needed for near tasks.
- Absence of significant posterior capsule opacity or other factors that could interfere with postoperative visual clarity.
Patients whose astigmatism is primarily lenticular rather than corneal may not experience the expected benefit from a toric IOL, since the correction targets corneal curvature specifically. Precise preoperative biometry, including corneal topography and keratometry, helps determine whether the astigmatism source is appropriate for toric correction.
For many patients with moderate to high corneal astigmatism, toric IOLs represent one of the most reliable ways to achieve sharp distance vision without glasses after cataract surgery. Accurate preoperative measurements and a thorough eye examination form the foundation for determining whether this lens is the right fit, a process that the next section explores in detail.
What Measurements and Tests Help Determine the Best Lens for You?
The measurements and tests that help determine the best lens for you include ocular biometry, corneal topography, optical coherence tomography, and advanced IOL power calculation formulas. These preoperative assessments guide your surgeon toward the most accurate lens selection.
Ocular biometry measures the eye’s axial length, anterior chamber depth, and lens thickness. These dimensions are essential inputs for IOL power calculations, which determine the correct lens strength needed to achieve your target refractive outcome. Modern optical biometers use laser interferometry to capture these values with high precision.
Corneal topography maps the curvature and shape of the cornea’s surface. This test identifies irregular astigmatism, corneal scarring, or other surface abnormalities that may affect premium IOL performance. For patients considering toric IOLs, topography confirms the magnitude and axis of astigmatism requiring correction.
Optical coherence tomography (OCT) scans the retina and macula to detect conditions that could limit visual outcomes. A healthy macula is critical for multifocal and extended depth of focus IOLs, since these lenses distribute light across multiple focal points and rely on optimal retinal function.
Once biometric data is collected, surgeons apply IOL power calculation formulas to determine the ideal lens strength. According to a study published in Clinical Ophthalmology, the Kane formula was found to be the most accurate among five new-generation IOL power formulas in terms of mean absolute error and median absolute error. AI-driven formulas like Hill-RBF 3.0 have also demonstrated comparable or superior predictive accuracy, giving surgeons additional tools for precise lens selection.
The accuracy of these preoperative measurements directly shapes postoperative visual quality. Even small errors in biometry or formula selection can result in a refractive surprise, where the patient’s vision after surgery does not match the intended target. This is why thorough, multi-layered testing before cataract surgery is not optional; it is foundational to achieving the best possible outcome with any IOL type.
Understanding which tests your surgeon plans to perform can help you feel more prepared for your preoperative evaluation and the lens decision that follows.
What Are the Potential Benefits of Premium IOLs Over Standard Lenses?
The potential benefits of premium IOLs over standard lenses include reduced dependence on glasses, correction of astigmatism, and an extended range of clear vision across multiple distances.
Standard monofocal lenses provide excellent clarity at one focal point, typically distance. Premium IOLs build on that foundation by addressing limitations that monofocal designs leave unresolved. The specific advantage depends on the lens category:
- Broader range of functional vision. Multifocal and extended depth of focus IOLs may allow patients to see clearly at distance, intermediate, and near ranges without switching between prescription eyewear.
- Astigmatism correction built into the implant. Toric IOLs can correct pre-existing corneal astigmatism at the time of cataract surgery, potentially eliminating the need for astigmatism-correcting glasses afterward.
- Reduced reliance on reading glasses. Presbyopia-correcting designs, such as trifocal and EDOF lenses, target the near and intermediate zones that monofocal lenses do not address.
- Post-surgical fine-tuning. The Light Adjustable Lens allows power adjustments after implantation using UV light, offering a level of customization unavailable with fixed-power alternatives.
According to a meta-analysis published in the National Library of Medicine, trifocal IOLs performed better than hybrid multifocal-EDOF IOLs at near vision, while both lens categories achieved high levels of patient satisfaction.
These advantages do come with trade-offs. Not every patient benefits equally from premium technology, and lifestyle goals should guide the decision. For many candidates, however, the practical gains in spectacle independence represent a meaningful improvement in daily quality of life.
Understanding the potential risks and side effects of premium IOLs is equally important before making a final choice.
What Are the Possible Risks or Side Effects of Premium IOLs?
The possible risks or side effects of premium IOLs include visual disturbances, lens misalignment, and neuroadaptation challenges. The sections below cover each risk category in detail.
What Visual Disturbances May Occur With Multifocal IOLs?
Visual disturbances that may occur with multifocal IOLs include halos, glare, and starbursts around light sources, particularly at night. These photic phenomena result from the way multifocal optics split light across multiple focal points.
Not all premium designs carry the same risk. According to a 2024 review in the National Center for Biotechnology Information, EDOF IOLs exhibit higher contrast sensitivity than trifocal IOLs at lower spatial frequencies, with a lower incidence of photic phenomena. Patients implanted with EDOF lenses may, however, experience worse near vision compared to multifocal groups.
For most patients, these disturbances diminish over the first several months as the brain adapts. Still, anyone who frequently drives at night or works in low-light conditions should discuss photic phenomena risk with their surgeon before selecting a multifocal design.
What Risks Are Associated With Toric IOL Misalignment?
The risks associated with toric IOL misalignment include residual astigmatism and reduced uncorrected distance vision. Toric lenses must remain precisely aligned with the corneal astigmatism axis to deliver their full corrective benefit; even a few degrees of rotation can diminish visual outcomes.
Misalignment may occur during the early postoperative period if the lens rotates within the capsular bag before it stabilizes. When significant rotation is detected, a secondary repositioning procedure may be necessary. Factors such as a large capsular bag or incomplete lens fixation can increase rotation risk. For this reason, thorough preoperative biometry and careful surgical technique are essential to achieving stable toric IOL positioning.
How May Neuroadaptation Challenges Affect Premium IOL Outcomes?
Neuroadaptation challenges may affect premium IOL outcomes by prolonging the period needed for the brain to adjust to a new optical system. Multifocal and EDOF lenses distribute light differently than the natural crystalline lens, requiring the visual cortex to relearn how it processes simultaneous focal points.
Most patients adapt within three to six months. During this window, mild visual symptoms, such as reduced contrast or difficulty switching focus between distances, are common. Patients with a history of highly precise visual demands or those accustomed to single-vision correction may find this adjustment period more noticeable.
Setting realistic expectations before surgery is one of the most effective ways to improve satisfaction during neuroadaptation. With an understanding of premium IOL risks, patients can make more informed decisions about the costs and coverage options associated with each lens type.
How Does Cost Differ Among IOL Options and What May Insurance Cover?
Cost differs among IOL options based on whether the lens is classified as standard or premium, and insurance coverage varies accordingly. Below is what patients should know about out-of-pocket expenses and Medicare policies for different lens categories.
Standard monofocal IOLs are typically covered by Medicare and most private insurance plans as part of medically necessary cataract surgery. Premium lenses, including multifocal, extended depth of focus, toric, and light adjustable options, carry additional out-of-pocket fees because insurers classify them differently.
According to an economic evaluation published in Translational Vision Science & Technology, the average out-of-pocket cost for cataract surgery, including lens replacement, is estimated at $4,131 per eye. Premium IOL upgrades can increase this figure significantly, as the added technology cost falls entirely on the patient.
Medicare does not cover the additional costs of presbyopia-correcting IOLs or astigmatism-correcting IOLs, as the Centers for Medicare & Medicaid Services does not consider these upgrades medically necessary. Medicare will cover the base surgical procedure and a standard monofocal lens, but patients choosing a premium option pay the difference between the standard and upgraded lens.
This cost structure makes it essential to discuss both clinical goals and financial planning with your surgical team before selecting a lens. Understanding what insurance will and will not cover helps patients set realistic expectations and avoid unexpected expenses during the decision-making process.
What Questions Should You Ask Your Surgeon Before Choosing a Lens?
The questions you should ask your surgeon before choosing a lens cover your eye health history, lifestyle vision goals, lens-specific trade-offs, and out-of-pocket costs. Preparing these questions supports shared decision-making and helps match the right IOL to your individual needs.
According to a 2024 study published in Patient Education and Counseling, use of a Patient Decision Aid for IOL selection significantly improves patient preparation and enhances the level of shared decision-making between patients and clinicians. Bringing a structured set of questions to your preoperative consultation can make the conversation more productive, ensuring nothing important is overlooked.
Key questions to ask before your cataract lens selection include:
- Am I a candidate for premium IOLs? Ask whether any existing conditions, such as glaucoma, macular degeneration, or corneal irregularities, may limit your options.
- Which lens type best fits my daily activities? Discuss whether distance vision, intermediate vision, or near vision matters most for your routine.
- What visual side effects should I expect? Inquire about the likelihood of halos, glare, or reduced contrast sensitivity with each lens option.
- How accurate are my preoperative measurements? Understanding the biometry results and the formula used for lens power calculation can help set realistic expectations.
- What will I pay out of pocket? Clarify which costs Medicare or private insurance covers and what the upgrade fee is for any premium lens.
- What happens if I am not satisfied with my vision after surgery? Ask about enhancement options, lens exchange timelines, and when glasses may still be needed.
Patients who treat the lens consultation as a two-way conversation tend to feel more confident in their final choice. With these questions prepared, surgeon-reviewed resources can further clarify each option.
How Can Surgeon-Reviewed Guidance Help You Choose the Right IOL?
Surgeon-reviewed guidance can help you choose the right IOL by translating complex clinical data into clear, actionable information tailored to your vision goals and eye health. The following sections cover how Eye Surgery Today supports your decision and the key takeaways for choosing a lens after cataract surgery.
Can Eye Surgery Today Help You Understand Your IOL Options?
Yes, Eye Surgery Today can help you understand your IOL options. As a surgeon-reviewed education platform, Eye Surgery Today provides clear, unbiased guides covering every major lens category, from monofocal and multifocal IOLs to toric, extended depth of focus, and light adjustable lenses. Each guide breaks down how a lens works, who may benefit most, and what potential trade-offs to consider. Our comprehensive resources also include specific guidance on IOL implants for children with cataracts, addressing their unique developmental needs. Rather than replacing the conversation with your surgeon, these resources prepare you to ask better questions and evaluate recommendations with confidence. Drawing on sources such as Cataract & Refractive Surgery Today Europe, Eye Surgery Today distills peer-reviewed findings into language that does not require a medical background to understand. For patients navigating a decision that affects daily vision for years to come, having access to surgeon-reviewed content can be the difference between feeling overwhelmed and feeling informed.
What Are the Key Takeaways About Choosing the Right Lens After Cataract Surgery?
The key takeaways about choosing the right lens after cataract surgery center on matching your lifestyle, eye health, and budget to the IOL that best fits your needs. Several core principles should guide this decision:
- No single IOL is ideal for every patient; each lens type involves trade-offs between range of vision, visual clarity, and potential side effects.
- Photic phenomena such as halos and glare are more pronounced in presbyopia-correcting IOLs than in monofocal IOLs, which can cause dissatisfaction if expectations are not set in advance.
- Cost plays a significant role. According to a study published in Translational Vision Science & Technology, the average out-of-pocket cost for cataract surgery, including lens replacement, is estimated at $4,131 per eye.
- Pre-existing conditions, including glaucoma, macular degeneration, and corneal irregularities, may limit premium IOL candidacy.
- Shared decision-making with your surgeon, informed by accurate biometry and a thorough eye exam, produces the best outcomes.
The most empowered patients are those who understand both the possibilities and the limitations of each lens option before entering the operating room. Investing time in surgeon-reviewed educational resources helps bridge the gap between clinical complexity and confident, informed consent.





