Toric lenses are specialized intraocular lenses (IOLs) that feature different refractive powers in specific places, designed to correct corneal astigmatism during cataract surgery through cylindrical power and precise axis alignment.
This guide covers the optical mechanics behind toric lens correction, the available lens categories and candidacy criteria, preoperative measurement and surgical planning, potential benefits and risks, and how toric IOLs compare to alternative astigmatism treatments.
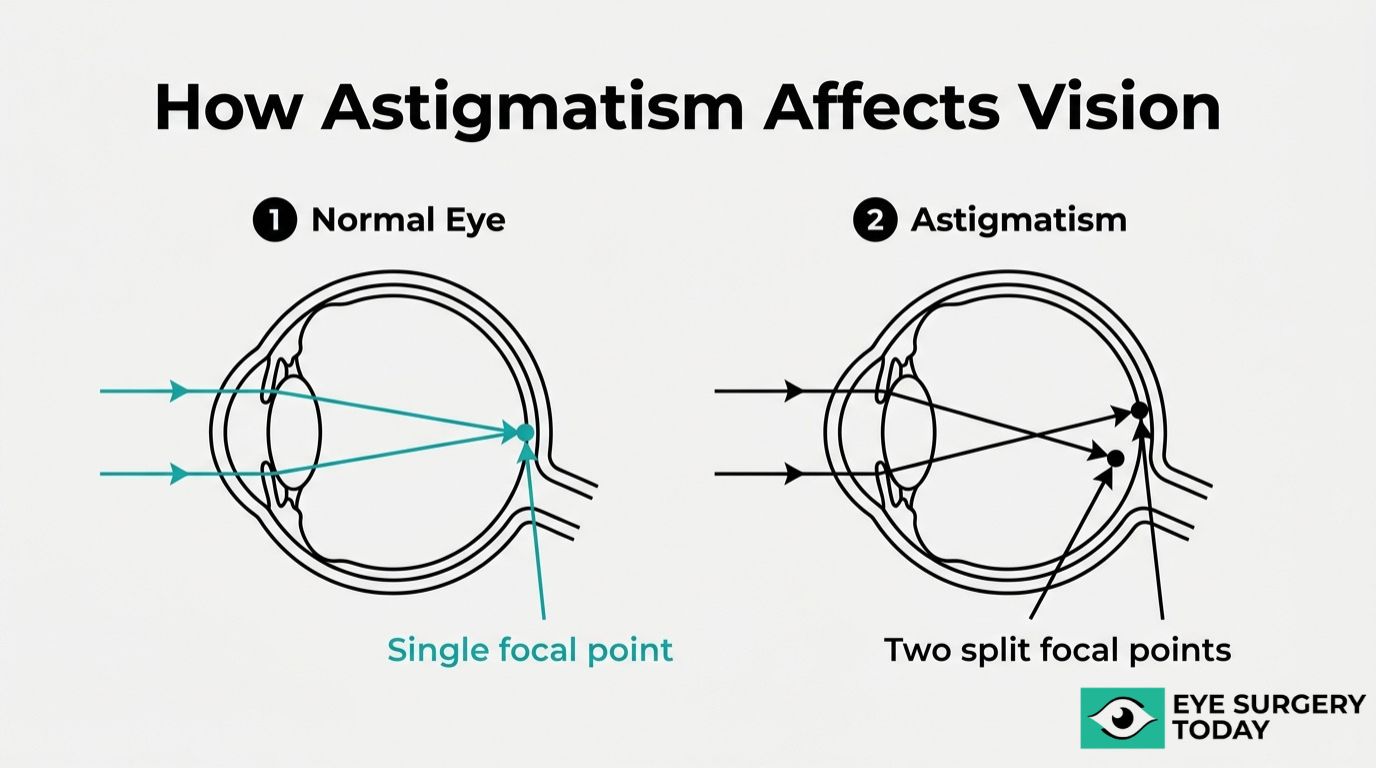
Astigmatism occurs when the cornea curves more steeply in one direction than the other, preventing light from converging to a single focal point on the retina. Toric IOLs neutralize this irregular curvature by matching their cylindrical axis to the eye’s steepest meridian, and even small misalignments can significantly reduce corrective efficacy.
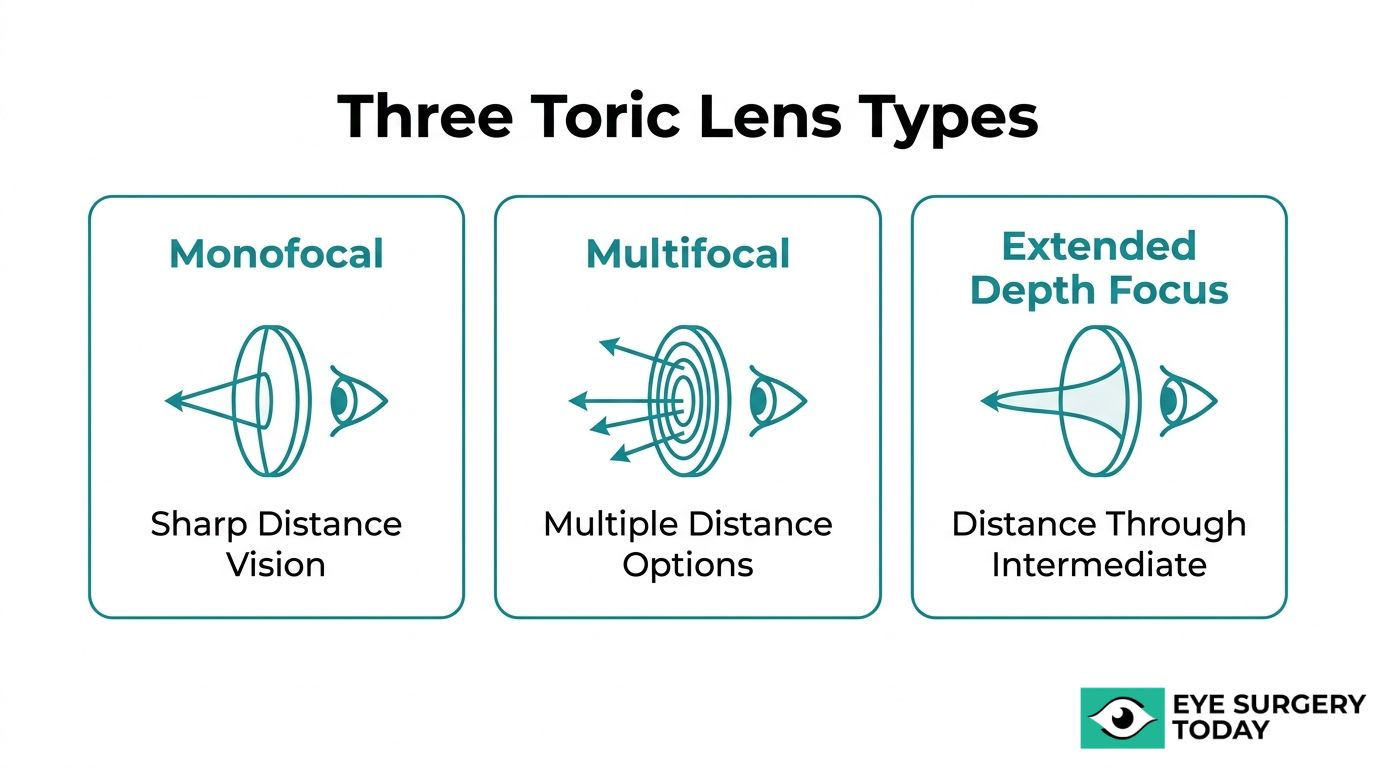
Toric lenses are available in monofocal, multifocal, and extended depth of focus designs. Monofocal versions provide sharp distance vision with minimal optical side effects, multifocal options may reduce glasses dependence across multiple distances, and EDOF lenses stretch a continuous focal range from distance through intermediate vision.
Candidacy depends on the type, regularity, and magnitude of corneal astigmatism. Clinical thresholds help surgeons determine when a toric IOL offers meaningful benefit over a standard lens, while conditions such as irregular astigmatism or progressive corneal disease may limit eligibility.
Preoperative corneal topography, modern toric calculators that account for posterior corneal contributions, and image-guided axis marking systems all contribute to surgical precision. These planning tools help minimize residual astigmatism and support predictable visual outcomes.
Compared to limbal relaxing incisions, toric IOLs may deliver more consistent astigmatism reduction. They also address the refractive error in a single surgical step, which can be more efficient than relying on post-operative LASIK enhancement.
What Is Astigmatism and How Does It Affect Vision?
Astigmatism is a refractive error where light entering the eye does not converge to a single focal point on the retina, causing blurred or distorted vision at all distances. According to StatPearls (NCBI Bookshelf), Astigmatism can be categorized as corneal (abnormal corneal curvature, position, or refractive index), lenticular (abnormal lens curvature, position, or refractive index), or retinal (oblique placement of the macula) according to StatPearls, although retinal and lenticular contributions are often grouped clinically as internal astigmatism. Rather than a perfectly round shape, the affected cornea or lens is curved more steeply in one meridian than the other, somewhat like a football compared to a basketball. This irregular curvature creates two competing focal points, which is why people with uncorrected astigmatism often experience symptoms such as:
- Blurred vision at both near and far distances
- Eye strain and headaches, especially after prolonged reading
- Difficulty seeing clearly at night or in low-light conditions
- Squinting to bring objects into focus
Because astigmatism distorts light before it reaches the retina, standard spherical lenses alone cannot fully correct it. Choosing the right lens, particularly during cataract surgery, requires accounting for this asymmetric curvature to restore sharp, focused vision.
Why Does Astigmatism Matter During Lens Selection?
Astigmatism matters during lens selection because uncorrected corneal irregularity can persist after surgery, reducing visual clarity even with an otherwise successful implant. Choosing the right lens type and power depends on the degree and axis of astigmatism present before the procedure.
When astigmatism goes unaddressed during cataract surgery, light continues to split into multiple focal points rather than converging on a single point on the retina. A standard monofocal IOL, which has uniform power across its surface, cannot compensate for the uneven curvature that causes this refractive error. The result is often residual astigmatism that leaves patients dependent on glasses for distance vision, undermining one of the primary goals of modern lens replacement.
This is why preoperative astigmatism measurements directly shape the surgical plan. The orientation of astigmatism, whether with-the-rule, against-the-rule, or oblique, influences both the lens model selected and the axis at which it must be positioned. For patients with clinically significant astigmatism, toric IOLs offer a purpose-built solution, though precise candidate selection and fitting are essential for optimal outcomes.
Understanding how toric lenses achieve this correction starts with their unique optical design.
How Do Toric Lenses Work to Correct Astigmatism?
Toric lenses work to correct astigmatism by using different refractive powers along specific meridians, compensating for the uneven curvature of the cornea. The following sections explain how the toric design differs from standard lenses and why precise alignment is essential.
How Does the Toric Lens Design Differ From Standard Lenses?
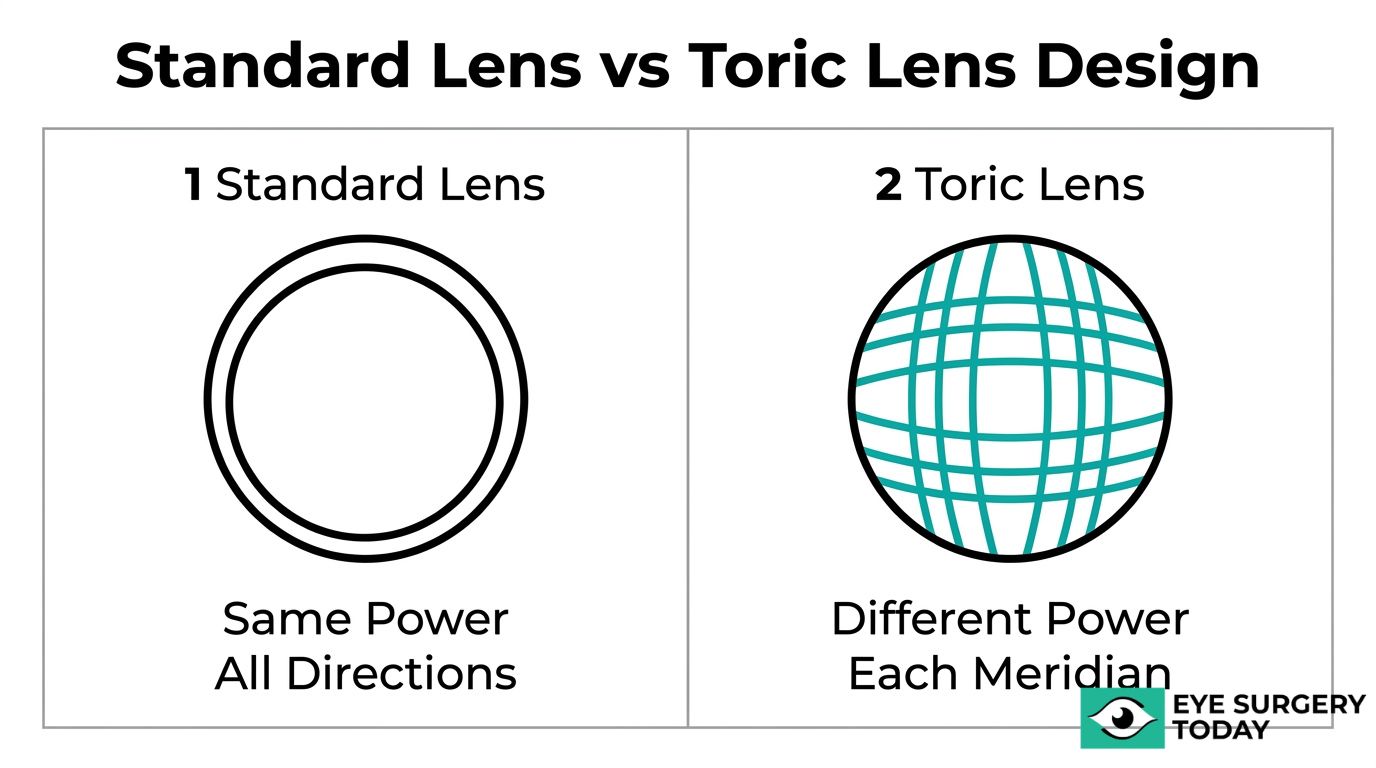
The toric lens design differs from standard lenses by incorporating cylindrical power across different meridians rather than uniform power throughout. Standard monofocal IOLs provide a single refractive power that corrects for distance but cannot address the directional variation in focus caused by astigmatism.
Astigmatism occurs when parallel rays of light passing through the cornea do not converge to a single point on the retina. This irregularity can be corneal, lenticular, or retinal in origin. Because a standard lens treats the eye as though its curvature is symmetrical, it leaves astigmatic error uncorrected.
Toric IOLs solve this by featuring different refractive powers in different places, paired with precise axis alignment. This cylindrical power directly counteracts the corneal curvature mismatch that causes blurred or distorted vision. For patients undergoing cataract surgery, this design distinction is what separates a lens that merely replaces the clouded natural lens from one that simultaneously corrects a pre-existing refractive error.
How Does Toric Lens Alignment Correct Corneal Irregularity?
Toric lens alignment corrects corneal irregularity by positioning the lens’s cylindrical axis to match the steep meridian of the cornea exactly. When the axis is properly aligned, the lens neutralizes the asymmetric curvature that scatters light unevenly across the retina.
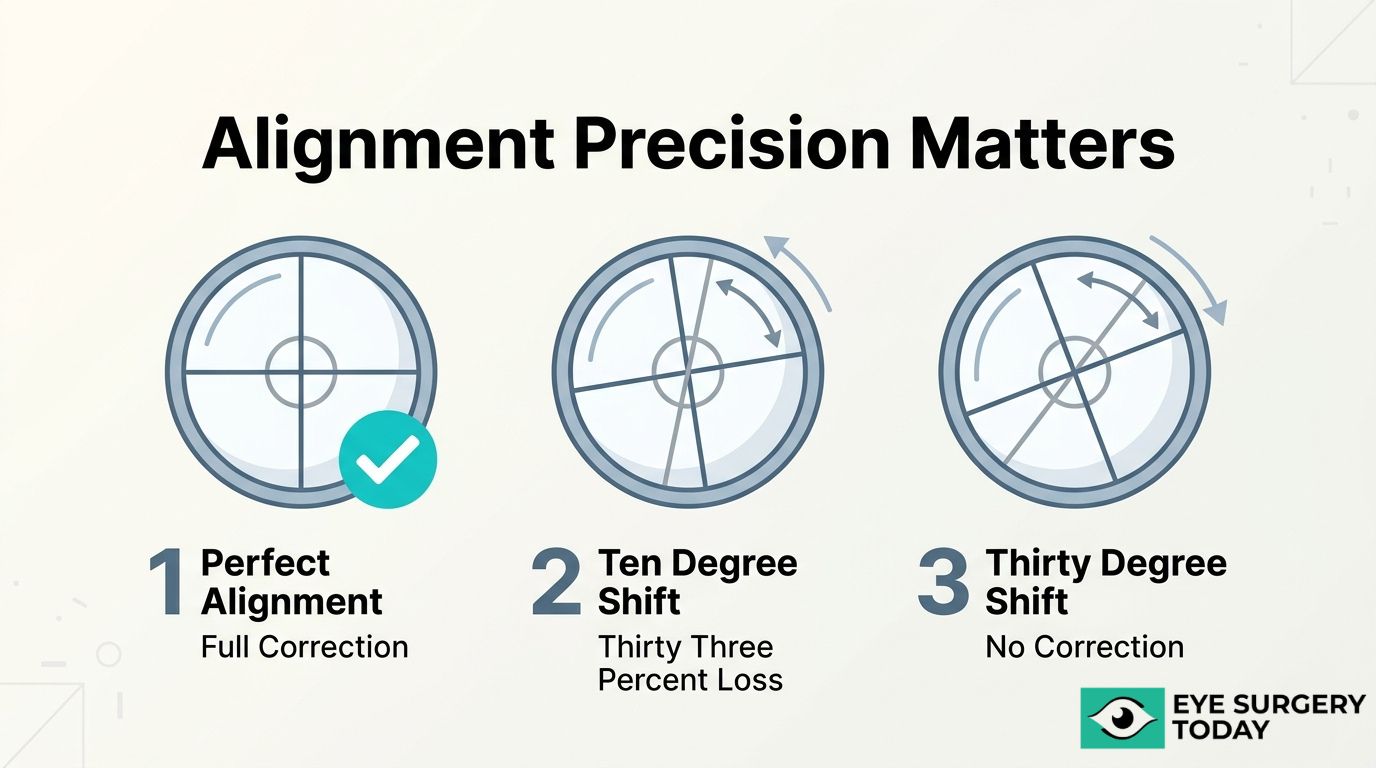
Precision here is not optional. According to a study published in Frontiers in Medicine (2024), a misalignment of just 10 degrees results in a 33% loss of astigmatism-correcting efficacy, while a 30-degree misalignment can fail to correct astigmatism entirely or even introduce it on a new axis. These narrow tolerances explain why surgeons rely on advanced marking techniques and image-guided systems during implantation.
Clinical evidence supports this need for accuracy. A prospective study of the AT TORBI 709M bitoric monofocal IOL, involving 51 eyes in 31 patients, confirmed the lens is both effective and safe when properly aligned for correcting hyperopia and astigmatism. Rotational stability after placement is equally critical, as even small postoperative shifts can meaningfully reduce visual outcomes.
Understanding how alignment drives toric lens performance helps clarify the types of toric lenses available today.
What Types of Toric Lenses Are Available?
The types of toric lenses available are monofocal, multifocal, and extended depth of focus (EDOF) designs. Each category combines astigmatism correction with a different focal strategy.
Toric Monofocal Lenses
Toric monofocal lenses correct astigmatism while providing clear vision at one fixed distance, typically far. These lenses remain the most widely implanted toric option during cataract surgery because they deliver sharp distance vision with a straightforward optical design.
Patients who choose toric monofocal lenses can expect excellent clarity for activities like driving, though reading glasses are usually still needed for near tasks. Because the optics involve a single focal point, visual side effects such as halos or glare tend to be minimal compared to multifocal alternatives.
For patients whose primary concern is reducing dependence on distance glasses while correcting astigmatism, toric monofocal lenses often represent the most reliable starting point in the decision-making process.
Toric Multifocal Lenses
Toric multifocal lenses correct astigmatism while simultaneously providing clear vision at multiple distances, including near, intermediate, and far. This dual functionality can significantly reduce the need for glasses after cataract surgery.
The multifocal design splits incoming light into distinct focal zones. While this approach broadens the range of functional vision, it may introduce visual phenomena such as halos or glare around lights at night. Patients with active lifestyles who want minimal glasses dependence across all distances are often the best candidates for this lens category.
Not every patient tolerates the light-splitting optics equally well. A thorough preoperative discussion with an ophthalmologist helps determine whether a toric multifocal design aligns with individual visual demands and tolerance for potential trade-offs.
Toric Extended Depth of Focus Lenses
Toric extended depth of focus lenses correct astigmatism while stretching a single elongated focal point to cover distance and intermediate vision. Unlike multifocal designs that create separate focal zones, EDOF technology produces a continuous range of focus, which may reduce halos and glare.
According to the American Academy of Ophthalmology, the FDA approved the Tecnis Symfony Toric IOL in July of 2016, as the first EDOF toric lens indicated for adult cataract patients with greater than or equal to 1 D of pre-existing corneal astigmatism. This approval established EDOF toric technology as a distinct clinical category.
EDOF toric lenses are particularly well suited for patients who prioritize smooth distance-to-intermediate vision with fewer optical disturbances than multifocal lenses, though near reading glasses may still be needed for fine print.
With the right lens category identified, the next step is determining whether your eyes meet the criteria for toric implantation.
Who Is a Good Candidate for Toric Lenses?
A good candidate for toric lenses is typically a cataract surgery patient with regular corneal astigmatism above a clinically meaningful threshold. Candidacy depends on astigmatism severity, corneal regularity, and overall ocular health.
Can Patients With Mild Astigmatism Benefit From Toric Lenses?
Patients with mild astigmatism can benefit from toric lenses, though the decision depends on the type and magnitude of astigmatism present. Not every mild case warrants a toric IOL, because posterior corneal astigmatism may partially offset the anterior component on its own.
The Baylor Nomogram, published by the American Academy of Ophthalmology, recommends a threshold of 1.7 D of anterior corneal astigmatism before selecting a toric IOL in patients with with-the-rule astigmatism, accounting for an average posterior corneal astigmatism of −0.30 D. Below that threshold, the residual astigmatism after standard IOL implantation may already fall within a visually acceptable range.
Still, when mild astigmatism does exceed the clinical threshold, toric IOLs can deliver measurable gains. A 1-year randomized clinical trial involving 517 patients found that the AcrySof Toric IOL effectively reduced residual refractive astigmatism and improved uncorrected distance visual acuity compared to standard monofocal IOLs. For patients near the borderline, a detailed discussion with the surgeon helps weigh whether the added precision of a toric lens justifies the selection.
Are Toric Lenses Suitable for Patients With High Astigmatism?
Toric lenses are suitable for patients with high astigmatism, provided accurate preoperative measurements guide lens power and axis selection. Higher astigmatism introduces greater variability in posterior corneal contribution, which makes precise calculation essential.
According to studies in the American Journal of Ophthalmology, the Barrett Toric Calculator demonstrates comparable prediction accuracy for residual refractive astigmatism when using estimated versus measured posterior corneal astigmatism, with no significant differences in prediction error between methods. This has clinical relevance because it supports the use of modern toric calculators even when direct PCA measurements may not be available.
In practice, high-astigmatism patients often stand to gain the most from toric lens implantation, since standard monofocal IOLs leave substantial uncorrected curvature that typically requires thick spectacle lenses or additional procedures.
What Conditions May Disqualify Someone From Toric Lenses?
The conditions that may disqualify someone from toric lenses include irregular corneal astigmatism, progressive corneal disease, and unstable refractive measurements. Toric IOLs correct regular astigmatism along predictable meridians, so irregular patterns undermine their effectiveness.
Specific disqualifying factors include:
- Keratoconus or pellucid marginal degeneration, which cause irregular corneal curvature that a toric IOL cannot adequately address.
- Prior corneal refractive surgery with irregular healing, where unpredictable corneal shape compromises toric power calculations.
- Significant dry eye disease, which distorts keratometry and topography readings used for lens selection.
- Zonular instability or pseudoexfoliation syndrome, which may increase the risk of postoperative lens rotation.
- Fuchs endothelial dystrophy at an advanced stage, where corneal edema alters refractive measurements and may require future corneal procedures.
Patients with any of these conditions should discuss alternative astigmatism management strategies with their ophthalmologist before proceeding with lens selection. Understanding candidacy criteria early helps set realistic expectations for visual outcomes after cataract surgery.
What Are the Potential Benefits of Toric Lenses?
The potential benefits of toric lenses include sharper uncorrected distance vision, reduced dependence on glasses after surgery, and more precise astigmatism correction compared to alternative techniques.
Toric IOLs correct corneal astigmatism at the time of cataract surgery, addressing two vision problems in a single procedure. Standard monofocal lenses leave pre-existing astigmatism untreated, which often means patients still need corrective eyewear for clear distance vision afterward. By incorporating cylindrical power matched to the patient’s specific corneal curvature, toric lenses can neutralize the refractive imbalance that astigmatism creates.
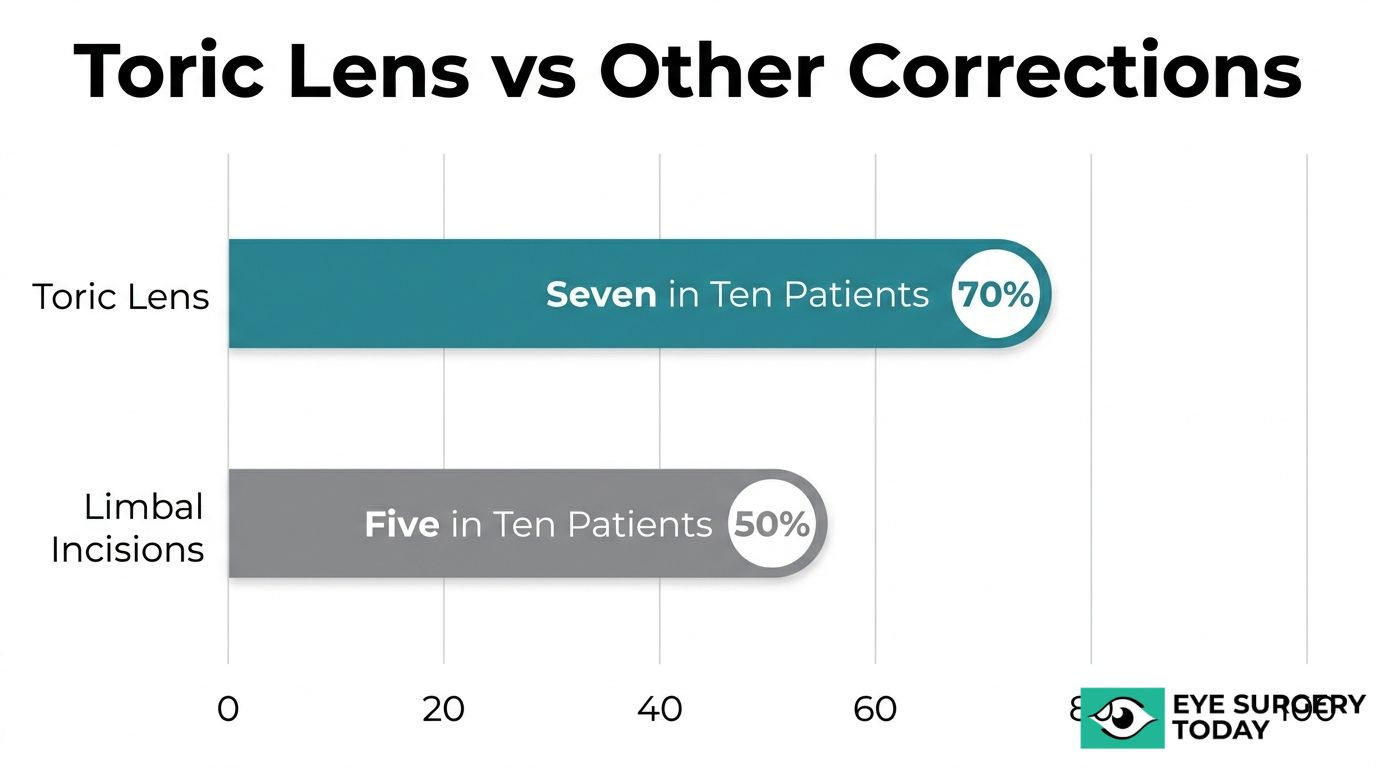
A Cochrane systematic review of 10 randomized controlled trials covering 626 eyes found that patients receiving toric IOLs were more likely to achieve residual refractive astigmatism of less than 0.5 D (700 per 1,000) compared to those receiving limbal relaxing incisions (500 per 1,000). This level of correction often translates into functional independence from distance glasses for daily activities.
For patients with moderate to high corneal astigmatism, toric lenses may offer the most predictable refractive outcome available during cataract surgery. The correction is built into the implant itself, so it does not depend on corneal healing patterns the way incisional techniques do. From a clinical standpoint, this built-in stability makes toric IOLs one of the most reliable tools for managing astigmatism during lens replacement.
Understanding these benefits is only part of the decision; knowing the possible risks helps complete the picture.
What Are the Possible Risks and Complications of Toric Lenses?
The possible risks and complications of toric lenses include postoperative lens rotation, residual astigmatism, and long-term misalignment. Each complication can reduce the lens’s corrective effectiveness.
What Happens If a Toric Lens Rotates After Surgery?
If a toric lens rotates after surgery, its astigmatism-correcting power shifts off the intended axis, reducing visual clarity. Toric IOLs depend on precise axis alignment to neutralize corneal astigmatism. Even modest rotational displacement compromises this correction significantly.
According to a 2024 study published in Frontiers in Medicine, a misalignment of just 10 degrees results in a 33% loss of astigmatism-correcting efficacy, while a 30-degree misalignment can fail to correct astigmatism entirely or even introduce it on a new axis.
Rotation most commonly occurs within the first 24 to 48 hours after implantation, before the lens fully stabilizes inside the capsular bag. If clinically significant rotation is detected, the surgeon may recommend a brief repositioning procedure to realign the lens to its target meridian. In practice, most modern toric IOL designs feature enhanced haptic stability that minimizes this risk considerably.
Can Residual Astigmatism Occur After Toric Lens Implantation?
Yes, residual astigmatism can occur after toric lens implantation. Even with accurate preoperative measurements and proper lens selection, small amounts of uncorrected astigmatism may remain. Contributing factors include posterior corneal astigmatism that was not fully accounted for during planning, slight lens rotation, or minor biometric calculation variability.
A 1-year randomized clinical trial involving 517 patients found that while the AcrySof Toric IOL effectively reduced residual refractive astigmatism compared to standard monofocal IOLs, some degree of residual cylinder persisted in a portion of cases. When residual astigmatism is visually significant, options such as spectacle correction, contact lenses, or LASIK enhancement may help refine the outcome. This is why thorough preoperative planning remains one of the most important steps in minimizing postoperative surprises.
What Are the Risks of Lens Misalignment Over Time?
The risks of lens misalignment over time include gradual loss of astigmatic correction, increased visual blur, and potential need for secondary intervention. Although most toric IOLs achieve rotational stability within days of implantation, late misalignment can occasionally occur due to capsular bag contraction or fibrosis.
Capsular changes exert asymmetric forces on the lens haptics, which may slowly shift the IOL off its intended axis over months or years. Patients with conditions such as pseudoexfoliation syndrome or zonular weakness face higher susceptibility to late displacement. Regular postoperative follow-up allows early detection of any shift before it becomes visually significant. If meaningful misalignment develops, repositioning surgery or a lens exchange procedure can restore proper axis orientation.
Understanding these risks helps set realistic expectations before choosing a toric lens, and careful surgical planning plays a central role in minimizing complications.
How Are Toric Lenses Measured and Fitted Before Surgery?
Toric lenses are measured and fitted before surgery through corneal mapping, precise power calculations, and axis alignment planning. The following subsections cover corneal topography, lens power determination, and axis marking techniques.
What Role Does Corneal Topography Play in Toric Fitting?
Corneal topography plays a central role in toric fitting by mapping the curvature of the entire corneal surface to identify the location, type, and magnitude of astigmatism. This imaging technology captures thousands of data points across the cornea, producing a detailed color-coded map that reveals irregular curvature patterns invisible to standard refraction alone.
Surgeons rely on topography to distinguish regular astigmatism, which toric lenses correct effectively, from irregular astigmatism caused by conditions like keratoconus, which may disqualify a patient from toric implantation. Topographic data also confirms whether astigmatism follows a with-the-rule or against-the-rule pattern, directly influencing lens selection and surgical approach.
Without accurate topographic mapping, even the most advanced toric lens can underperform. Consistent, repeatable topography readings across multiple visits give surgeons the confidence that astigmatism measurements are stable enough to proceed with a toric IOL.
How Do Surgeons Determine the Correct Toric Lens Power?
Surgeons determine the correct toric lens power by combining biometric measurements with specialized toric calculators that account for both anterior and posterior corneal astigmatism. Optical biometry measures axial length, anterior chamber depth, and keratometry values, which feed into formulas that calculate the optimal spherical and cylindrical power for each patient.
Modern calculators, such as the Barrett Toric Calculator, factor in posterior corneal contributions that older formulas ignored. According to a study in the American Journal of Ophthalmology, the Barrett Toric Calculator showed comparable residual astigmatism prediction accuracy whether posterior corneal astigmatism was estimated or measured using devices such as the IOLMaster 700 or Pentacam HR, with no significant difference across methods.
This level of computational precision helps surgeons avoid overcorrection or undercorrection. Selecting the wrong toric power can leave patients with residual astigmatism that defeats the purpose of choosing a premium lens in the first place.
Why Is Accurate Axis Marking Critical for Toric Lenses?
Accurate axis marking is critical for toric lenses because even small rotational errors significantly reduce astigmatism correction. The cylindrical power of a toric IOL must align precisely with the steepest corneal meridian; any deviation diminishes the lens’s corrective effect.
Image-guided systems for toric IOL alignment, such as the Callisto eye or Verion, typically achieve mean deviations from the target axis of about 3–4°, compared to 5–6° with manual marking techniques. Digital image-guided systems overlay preoperative reference images onto the surgeon’s microscope view, eliminating parallax and cyclotorsion errors that manual ink marks cannot fully prevent.
For this reason, many surgeons now prefer intraoperative digital guidance over traditional marking methods. Precise axis alignment remains the single most controllable factor in determining whether a toric IOL delivers its full corrective potential, making this step one of the most consequential in the entire surgical workflow.
With measurement and fitting complete, understanding the surgical procedure itself helps clarify what to expect on the day of implantation.
What Should You Expect During Toric Lens Implant Surgery?
Toric lens implant surgery follows the same phacoemulsification technique as standard cataract surgery, with additional precision steps for astigmatism correction. The sections below cover procedural differences and recovery expectations. For a comprehensive understanding, patients often find it helpful to first learn what is cataract surgery in its general context before delving into specialized IOL options.
How Is the Procedure Different From Standard Cataract Surgery?
The procedure is different from standard cataract surgery primarily in the preoperative marking and intraoperative alignment steps required for astigmatism correction. Both surgeries use phacoemulsification to remove the clouded natural lens through a small corneal incision. However, toric lens implantation adds critical axis-specific steps that standard monofocal placement does not require.
Key differences include:
- The surgeon marks reference points on the cornea before surgery to identify the precise meridian where the toric lens must align.
- Image-guided systems or manual ink markers are used to ensure the lens cylindrical axis matches the preoperative plan.
- After inserting the toric IOL into the capsular bag or alternative location, the surgeon rotates it to the exact target axis before the procedure is complete.
- Final verification confirms alignment, since even small rotational errors can reduce the astigmatism-correcting effect.
According to a 1-year randomized clinical trial published in the Journal of Cataract & Refractive Surgery involving 517 patients, the AcrySof Toric IOL effectively reduced residual refractive astigmatism and improved uncorrected distance visual acuity compared to standard monofocal IOLs. This additional alignment precision is what makes the toric procedure slightly longer, though the overall surgical experience remains comparable for patients.
What Happens During Recovery After Toric Lens Placement?
Recovery after toric lens placement follows a timeline similar to standard cataract surgery, typically spanning four to six weeks for full visual stabilization. Most patients notice improved clarity within the first few days, though mild blurriness, light sensitivity, and slight discomfort are common initially.
Your ophthalmologist may recommend the following during recovery:
- Use prescribed antibiotic and anti-inflammatory eye drops to prevent infection and control swelling.
- Avoid rubbing the eye, which could shift the toric lens from its aligned position.
- Attend follow-up appointments within the first week so the surgeon can verify the lens remains on axis.
- Limit strenuous activity and heavy lifting for at least two weeks to reduce intraocular pressure changes.
Early postoperative visits are particularly important with toric lenses because lens rotation, even by a few degrees, can diminish astigmatism correction. If significant rotation is detected, a brief repositioning procedure may be recommended. For most patients, though, modern toric IOL designs maintain stable alignment throughout healing. Understanding these recovery steps can help you prepare for what comes next: comparing toric lenses against other astigmatism correction options.
How Do Toric Lenses Compare to Other Astigmatism Corrections?
Toric lenses compare to other astigmatism corrections by offering more predictable refractive outcomes during cataract surgery than alternatives like limbal relaxing incisions or post-operative LASIK enhancement. The following sections examine each comparison.
How Do Toric IOLs Compare to Limbal Relaxing Incisions?
Toric IOLs compare to limbal relaxing incisions by delivering a higher rate of precise astigmatism correction with greater predictability. LRIs involve small corneal cuts at the limbus to flatten the steeper meridian, while toric IOLs correct astigmatism internally through cylindrical power built into the lens itself.
According to a Cochrane systematic review of 10 randomized controlled trials (626 eyes), patients receiving toric IOLs achieved residual refractive astigmatism below 0.5 D at a rate of 700 per 1,000, compared to 500 per 1,000 for those receiving LRIs. Some surgeons reserve toric IOLs for cases exceeding 1.00 D of corneal astigmatism, while others set a personal threshold near 2.0 D when LRIs remain a viable alternative.
LRIs can still serve patients with lower levels of corneal astigmatism effectively, but their outcomes depend more heavily on individual healing response. For patients seeking the most consistent reduction in residual astigmatism, toric IOLs remain the stronger option in most clinical scenarios.
How Do Toric IOLs Compare to LASIK Enhancement?
Toric IOLs compare to LASIK enhancement by correcting astigmatism at the time of cataract surgery rather than requiring a separate corneal procedure afterward. LASIK enhancement reshapes the cornea post-operatively to reduce residual refractive error, including any astigmatism left uncorrected by a standard monofocal IOL or toric IOL.
Choosing a toric IOL addresses astigmatism in a single surgical step, which often eliminates the need for additional healing time, added cost, and the risks associated with a second procedure. LASIK enhancement, however, may still be appropriate when residual astigmatism is unexpected or when a toric IOL was not initially selected.
Corneal stability and adequate tissue thickness are prerequisites for LASIK candidacy, so not every post-cataract patient qualifies. In practice, selecting a toric IOL during the primary surgery tends to be more efficient and cost-effective for patients with known pre-existing astigmatism. LASIK enhancement serves best as a backup strategy rather than a first-line correction plan.
With these comparisons in mind, a thorough consultation can help determine the best approach for each patient’s needs.
How Can You Make a Confident Decision About Toric Lenses?
You can make a confident decision about toric lenses by understanding how they correct astigmatism, knowing whether you meet candidacy criteria, and consulting a qualified ophthalmologist. The sections below cover how Eye Surgery Today supports your research and the essential takeaways from this guide.
Can Eye Surgery Today Help You Understand Your Lens Options?
Yes, Eye Surgery Today can help you understand your lens options. As a physician-led education platform founded by nationally recognized ophthalmology key opinion leaders, Eye Surgery Today provides surgeon-verified guides on toric IOLs, monofocal lenses, multifocal lenses, Light Adjustable Lens (LAL), and extended depth of focus designs.
Eye Surgery Today translates complex topics, such as toric lens alignment, axis marking precision, and candidacy thresholds, into clear language that supports informed decision-making. The platform covers the full scope of lens selection for astigmatism, from preoperative measurements like corneal topography to postoperative recovery expectations.
For patients weighing toric lenses against alternatives like limbal relaxing incisions or LASIK enhancement, Eye Surgery Today offers unbiased, evidence-based comparisons. Choosing the right intraocular lens is one of the most consequential decisions in cataract surgery, and having access to surgeon-level insight before your consultation can meaningfully improve the quality of that conversation.
What Are the Key Takeaways About Toric Lenses for Astigmatism?
The key takeaways about toric lenses for astigmatism are:
- Toric IOLs feature different refractive powers in different meridians, correcting corneal astigmatism through cylindrical power and precise axis alignment.
- Accurate alignment is critical; even small rotations significantly reduce correction efficacy.
- Candidacy depends on the type and degree of astigmatism, with clinical thresholds guiding when a toric IOL offers meaningful benefit over standard lenses.
- Multiple lens categories exist that can be used with toric lenses, including monofocal, multifocal, and extended depth of focus designs, each suited to different visual goals.
- Toric IOLs have demonstrated stronger astigmatism reduction compared to limbal relaxing incisions in clinical trials.
- Preoperative planning tools, such as corneal topography and modern toric calculators, improve surgical precision and visual outcomes.
Patients who invest time understanding these factors are better positioned to ask the right questions during their surgical consultation. Eye Surgery Today provides the surgeon-led educational resources to support that preparation.
