Minimally invasive glaucoma surgery (MIGS) is a category of procedures defined by an ab interno approach, minimal tissue trauma, and a favorable safety profile compared to traditional filtration surgeries like trabeculectomy and tube shunts.
This guide covers the types of MIGS devices and how they work, candidacy and patient selection, benefits and possible risks, medication reduction potential, the procedural experience and recovery, and how MIGS compares to other glaucoma treatments.
MIGS procedures fall into distinct categories, including trabecular bypass microstents, canal-based systems, subconjunctival filtering devices, excisional goniotomy tools, and aqueous suppression techniques. Each targets a different part of the eye’s drainage anatomy to lower intraocular pressure through a specific mechanism.
Candidacy for MIGS typically favors patients with ocular hypertension or mild-to-moderate open-angle glaucoma, particularly those already scheduled for cataract surgery or struggling with daily eye drop adherence. Advanced glaucoma cases may still require traditional surgical approaches.
We explore how MIGS procedures may reduce medication burden, with some patients experiencing meaningful decreases in the number of prescribed drops following surgery. Recovery typically occurs within days to weeks, with vision stabilizing faster than after conventional filtration procedures.
The guide also compares MIGS to eye drops, selective laser trabeculoplasty, trabeculectomy, and tube shunts, helping clarify where each option fits within the glaucoma treatment continuum. Choosing the right MIGS procedure depends on disease severity, ocular anatomy, and individualized goals established with a glaucoma specialist.
How Does MIGS Differ From Traditional Glaucoma Surgery?
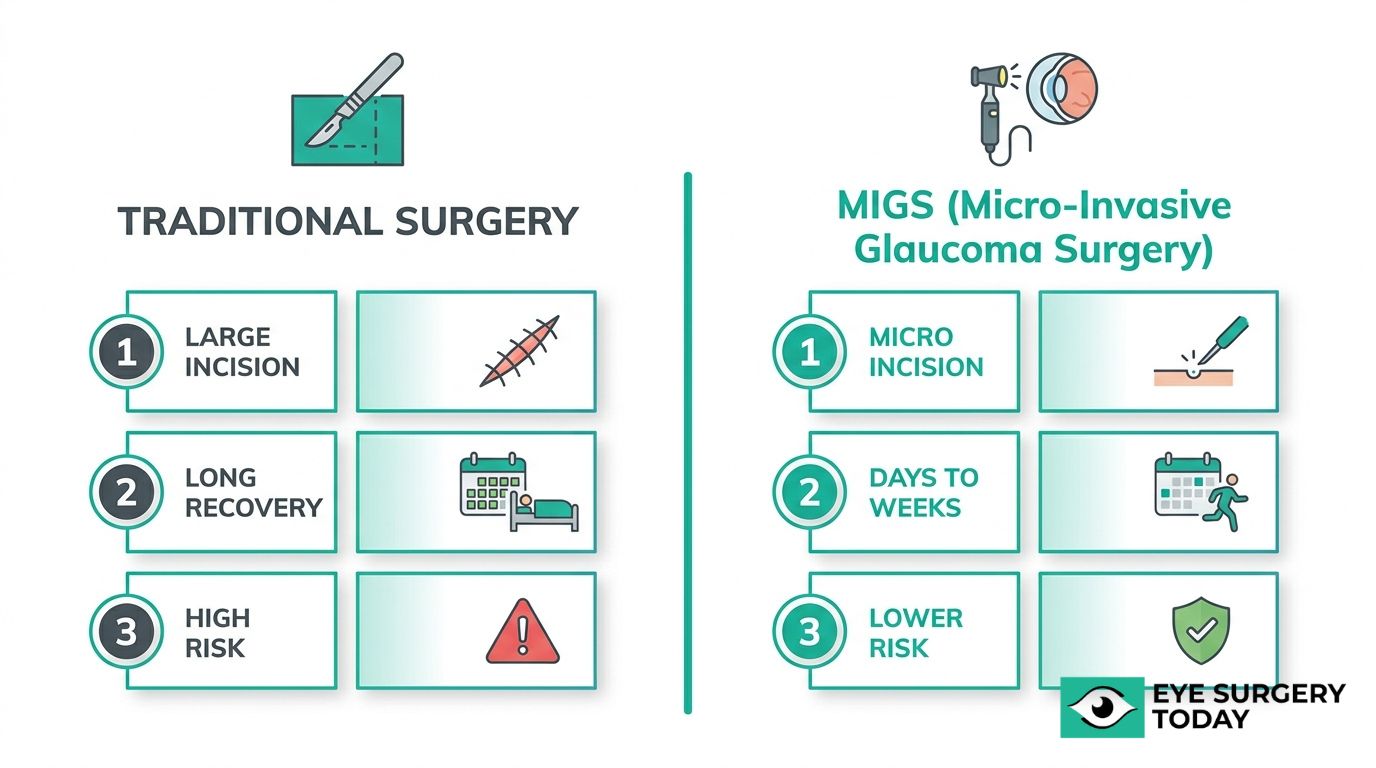
MIGS differs from traditional glaucoma surgery in surgical approach, tissue disruption, recovery time, and risk profile. The key distinctions involve how each method accesses the eye and the degree of structural alteration required.
Traditional glaucoma surgeries, such as trabeculectomy and tube shunt implantation, use an ab externo (from the outside) approach that requires significant conjunctival and scleral dissection. According to the American Academy of Ophthalmology, trabeculectomy involves creating a scleral flap and removing a portion of the trabecular meshwork to allow aqueous humor to drain into a subconjunctival bleb. This level of tissue manipulation can be highly effective for advanced glaucoma, but it carries a higher risk of complications, including bleb-related infections, hypotony, and prolonged recovery periods.
MIGS procedures, by contrast, use an ab interno (from the inside) approach through micro-incisions, preserving the conjunctiva and minimizing scleral disruption. Key differences include:
- Incision size: MIGS requires only micro-incisions, while traditional surgery needs larger conjunctival and scleral openings.
- Tissue trauma: MIGS causes minimal structural alteration; traditional procedures involve removing or bypassing significant tissue.
- Recovery time: MIGS recovery typically occurs within days to weeks, whereas traditional surgery may require months of monitoring and bleb management.
- Safety profile: MIGS carries a lower risk of serious postoperative complications compared to trabeculectomy or tube shunts.
- IOP reduction magnitude: Traditional surgeries generally achieve greater absolute IOP reduction, making them more suitable for advanced or refractory glaucoma.
- Combination potential: Many MIGS procedures can be performed alongside cataract surgery, reducing overall surgical burden.
This trade-off between safety and IOP-lowering power is what makes the choice between MIGS and traditional surgery so dependent on disease severity. For patients with mild-to-moderate glaucoma, the favorable risk profile of MIGS often makes it the more practical first surgical step. Understanding these procedural differences helps clarify which MIGS device types may be appropriate for specific clinical scenarios.
What Are the Types of MIGS Procedures?
The types of MIGS procedures include trabecular bypass microstents, canal-based systems, subconjunctival filtering devices, excisional goniotomy tools, and aqueous suppression techniques. The following sections cover each major device and approach.

iStent and iStent Inject
The iStent Trabecular Micro-Bypass Stent was the first MIGS device to receive FDA approval. The second-generation iStent inject contains two stents designed to enhance aqueous humor flow into Schlemm’s canal, offering broader trabecular bypass than its predecessor.
According to a 5-year real-world study of 271 eyes published in Ophthalmology and Therapy, iStent inject implantation reduced mean intraocular pressure from 16.4 mmHg to 13.7 mmHg, with mean medication count dropping from 2.24 to 0.62. That level of medication reduction can meaningfully improve daily quality of life for patients burdened by complex drop regimens. Both devices are typically implanted during cataract surgery through a single small corneal incision.
Hydrus Microstent
The Hydrus Microstent is a small, crescent-shaped scaffold placed directly into Schlemm’s canal. Unlike point-access devices, the Hydrus spans approximately three clock hours of the canal, dilating a larger segment to improve aqueous outflow through multiple collector channels. This broader canal engagement may offer a more consistent pressure-lowering effect in patients with mild-to-moderate open-angle glaucoma. The device is typically implanted alongside cataract surgery through a clear corneal approach.
Xen Gel Stent
The Xen Gel Stent is a soft, collagen-derived implant that creates a permanent drainage pathway from the anterior chamber to the subconjunctival space. Unlike trabecular bypass devices, the Xen bypasses the conventional outflow pathway entirely, functioning more like a miniaturized filtering procedure. This subconjunctival approach may benefit patients who need greater IOP reduction than trabecular devices alone can provide. Because it creates a filtering bleb, postoperative management sometimes includes antifibrotic agents to maintain bleb function.
Kahook Dual Blade Goniotomy
Kahook Dual Blade goniotomy is an excisional technique that removes a strip of trabecular meshwork rather than simply incising it. This clean excision may reduce tissue scarring and improve long-term aqueous access to Schlemm’s canal.
In a 6-year retrospective study of 90 eyes published in Ophthalmology and Therapy, the Kahook Dual Blade reduced mean intraocular pressure by 28.0% and decreased glaucoma medication use by 30.8%. The sustained IOP and medication reduction over six years makes this one of the more compelling tissue-removal options in the MIGS category. The procedure can be performed as a standalone surgery or combined with cataract extraction.
Trabectome
Trabectome is an electrosurgical device that ablates trabecular meshwork and the inner wall of Schlemm’s canal using controlled plasma energy. By removing the primary site of outflow resistance, Trabectome may enhance conventional aqueous drainage. The ab interno approach preserves the conjunctiva, which keeps future surgical options open if additional intervention becomes necessary. Trabectome can be performed as a standalone procedure or combined with phacoemulsification.
OMNI Surgical System
The OMNI Surgical System is a canal-based MIGS platform that performs both canaloplasty (viscodilation of Schlemm’s canal) and trabeculotomy through a single device. This dual-mechanism approach addresses outflow resistance at multiple points along the conventional pathway.
A systematic review and meta-analysis of 29 publications covering 2,379 eyes, published by Sight Sciences, found that the OMNI system achieved a treatment success rate (IOP reduction of 20% or greater) in approximately 89% of patients at 6, 12, and 24 months. The ability to combine viscodilation with trabeculotomy in one instrument gives surgeons flexibility to tailor the procedure to each patient’s anatomy.
Endocyclophotocoagulation (ECP)
Endocyclophotocoagulation (ECP) is a MIGS technique that reduces intraocular pressure by decreasing aqueous humor production rather than enhancing outflow. ECP uses endoscopic laser energy to selectively ablate ciliary body processes under direct visualization. Because the laser is applied internally with real-time imaging, energy delivery can be precisely controlled, which may lower the risk of over-treatment compared to external cyclophotocoagulation. ECP is frequently combined with cataract surgery and may be considered for patients who have not responded adequately to outflow-based procedures.
GATT (Gonioscopy-Assisted Transluminal Trabeculotomy)
GATT (Gonioscopy-Assisted Transluminal Trabeculotomy) is an ab interno procedure that uses a microcatheter or suture to perform a 360-degree trabeculotomy, opening the full circumference of Schlemm’s canal. This comprehensive approach addresses outflow resistance around the entire canal rather than a limited segment.
A 5-year study of 111 eyes published in the Journal of Glaucoma showed GATT reduced mean IOP from 30.3 mmHg to 17.5 mmHg, with medication count dropping from 3.8 to 2.2. These results suggest GATT may be particularly effective for patients presenting with higher baseline pressures, including some cases of moderate-to-advanced disease.
Understanding each device’s mechanism helps clarify how MIGS procedures lower eye pressure through different pathways.
How Does Each MIGS Procedure Work to Lower Eye Pressure?
Each MIGS procedure works to lower eye pressure by targeting one of three mechanisms: improving aqueous outflow, creating alternative drainage pathways, or reducing aqueous humor production. The following subsections explain how each approach functions.
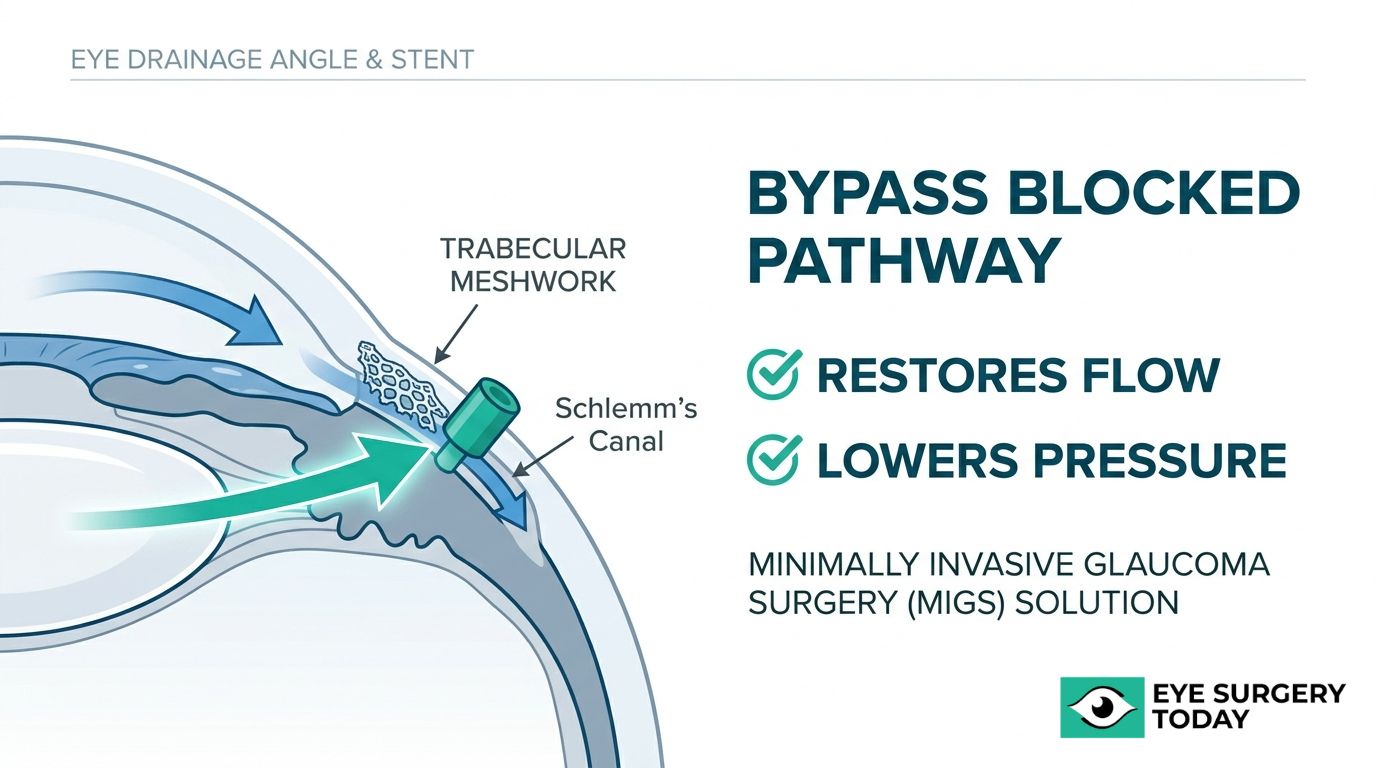
How Does Trabecular Bypass With Microstents Lower IOP?
Trabecular bypass with microstents lowers IOP by enhancing aqueous outflow through the conventional pathway, bypassing the trabecular meshwork. Tiny microstents, such as the iStent or Hydrus Microstent, are placed directly into Schlemm’s canal through an ab interno approach. Once positioned, these devices create a permanent opening that allows aqueous humor to flow freely past the area of greatest outflow resistance.
According to a systematic review of 401 studies (39,381 eyes) published between 2014 and 2024 in Clinical Ophthalmology, MIGS procedures generally lower IOP to the mid-teens in mild-to-moderate primary open-angle glaucoma, with trabecular bypass implants showing lower rates of serious adverse events compared to suprachoroidal devices. This favorable safety profile makes trabecular bypass one of the most practical first-line surgical options for patients with early-stage disease who need modest, reliable pressure reduction.
How Do Canal-Based Procedures Restore Natural Drainage?
Canal-based procedures restore natural drainage by reopening or expanding Schlemm’s canal and its collector channels. Techniques such as canaloplasty, viscodilation with the OMNI Surgical System, and gonioscopy-assisted transluminal trabeculotomy (GATT) work from inside the eye to address blockages along the conventional outflow pathway.
Rather than implanting a device, these procedures mechanically restore the eye’s existing drainage architecture. Viscoelastic material or a microcatheter dilates the full circumference of Schlemm’s canal, improving access to collector channels that may have collapsed or narrowed. Because canal-based approaches rely on the eye’s own anatomy, they can be particularly effective when the primary resistance sits within the canal system itself rather than at the trabecular meshwork alone.
How Do Suprachoroidal Shunts Create a New Drainage Path?
Suprachoroidal shunts create a new drainage path by facilitating aqueous humor drainage into the uveoscleral outflow pathway via the suprachoroidal space. A small implant is placed ab interno between the sclera and the choroid, redirecting fluid into a space that does not rely on the conventional trabecular outflow system.
This approach targets the uveoscleral pathway, which normally accounts for a secondary portion of total aqueous drainage. According to a report in the Journal of Ophthalmology, suprachoroidal MIGS devices reduce intraocular pressure specifically by channeling aqueous humor into this alternative route. Because the mechanism bypasses the trabecular meshwork entirely, suprachoroidal shunts may benefit patients whose conventional pathway is significantly compromised.
How Do Subconjunctival Filtering Devices Lower IOP?
Subconjunctival filtering devices lower IOP by creating a permanent drainage pathway from the anterior chamber to the subconjunctival space. The XEN Gel Stent, for example, is a soft gelatin tube inserted ab interno that channels aqueous humor beneath the conjunctiva, forming a small filtration bleb similar to what trabeculectomy produces.
This mechanism bypasses both the trabecular and uveoscleral outflow routes entirely, directing fluid to an external reservoir under the conjunctival tissue. Because subconjunctival devices create a bleb, they may achieve greater IOP reduction than trabecular or canal-based approaches. However, bleb-dependent procedures can require closer postoperative monitoring. For patients who need more aggressive pressure lowering than trabecular bypass alone can provide, subconjunctival filtering devices offer a minimally invasive alternative to traditional trabeculectomy.
How Does Reducing Aqueous Production With ECP Help?
Reducing aqueous production with ECP helps by decreasing the volume of fluid the eye generates, rather than improving its drainage. Endoscopic Cyclophotocoagulation uses laser energy delivered through an endoscopic probe to selectively ablate the ciliary body processes, which are the structures responsible for producing aqueous humor.
According to the American Glaucoma Society, ECP reduces intraocular pressure by targeting production at its source. Unlike drainage-based MIGS procedures, this approach can be effective even when outflow pathways are severely compromised. ECP is often performed alongside cataract surgery, allowing the surgeon to access the ciliary processes through the same incision. Because it does not depend on creating or maintaining a drainage channel, ECP may be especially useful for patients with refractory glaucoma or those who have not responded adequately to outflow-enhancing procedures.
Understanding how each mechanism targets a different part of the aqueous humor cycle can help patients discuss the most appropriate MIGS option with their ophthalmologist.
Who May Be a Good Candidate for MIGS?
Good candidates for MIGS typically include patients with mild to moderate glaucoma, those struggling with eye drop adherence, and individuals already scheduled for cataract surgery. The following subsections cover each candidate profile.
Can Patients With Mild to Moderate Glaucoma Benefit?
Patients with mild to moderate glaucoma can benefit significantly from MIGS. These procedures are specifically designed for this population, offering meaningful intraocular pressure reduction with a favorable safety profile.
Good candidates include patients with ocular hypertension or mild-to-moderate glaucoma who are eligible for local anesthesia, particularly those undergoing concomitant cataract surgery to reduce overall surgical burden and improve medication adherence. According to Dr. Inder Paul Singh, a board-certified ophthalmologist and President of The Eye Centers of Racine and Kenosha, “this interventional management strategy has enhanced the surgeon’s armamentarium for the treatment of mild to moderate glaucoma.”
Preoperative preparation typically involves optimizing the ocular surface and confirming candidacy, while postoperative recovery usually occurs within days to weeks. For patients in this disease stage, MIGS represents one of the most practical interventions available because it addresses both pressure control and quality of life before the disease progresses further.
Is MIGS Appropriate for Patients With Advanced Glaucoma?
MIGS is generally not considered a first-line surgical option for patients with advanced glaucoma. Most MIGS procedures target mild to moderate disease, and advanced cases often require more aggressive pressure reduction than standard MIGS devices typically deliver.
Refractory glaucoma, for certain MIGS criteria, is defined as prior failure of a filtering or cilioablative procedure, or uncontrolled intraocular pressure with progressive damage despite maximal tolerated medical therapy. Patients meeting this definition usually need trabeculectomy or tube shunt surgery. However, the 6th Edition of the European Glaucoma Society Guidelines, updated in 2026, includes new evidence-based guidance on integrating MIGS into the broader glaucoma treatment paradigm.
In select advanced cases, certain MIGS procedures may serve an adjunctive role. Your ophthalmologist can determine whether MIGS, traditional surgery, or a combination approach is most appropriate based on disease severity and treatment history.
Can MIGS Help Patients Who Struggle With Eye Drop Use?
MIGS can help patients who struggle with eye drop use by reducing or, in some cases, eliminating the need for daily glaucoma medications. Medication non-adherence is a well-recognized barrier to effective glaucoma management, and missed doses can allow intraocular pressure to remain elevated.
By creating new drainage pathways or enhancing existing outflow, MIGS procedures may lower eye pressure enough to decrease the number of prescribed drops. For patients with arthritis, dexterity limitations, or difficulty maintaining a consistent drop schedule, this reduction in medication burden can be especially meaningful. A healthcare provider can evaluate whether a specific MIGS procedure may help simplify a patient’s treatment regimen.
Are Patients Already Scheduled for Cataract Surgery Eligible?
Patients already scheduled for cataract surgery are often excellent candidates for MIGS. Many MIGS procedures are designed to be performed simultaneously with phacoemulsification, combining both interventions into a single operative session under the same anesthesia.
This combined approach offers several advantages:
- It reduces the total number of surgeries a patient undergoes.
- It may lower intraocular pressure while also restoring visual clarity from lens replacement.
- It can decrease postoperative medication burden, simplifying long-term glaucoma management.
For patients with coexisting cataracts and mild to moderate open-angle glaucoma, adding a MIGS procedure during cataract surgery is one of the most efficient strategies for addressing both conditions. This integrated approach is often employed in procedures such as laser cataract surgery, which also uses advanced technology to enhance precision and outcomes. Your ophthalmologist can assess whether the timing and type of MIGS procedure align with your cataract surgery plan.
Understanding candidacy is one part of the decision; knowing what MIGS may offer next helps set realistic expectations.
What Are the Potential Benefits of MIGS?
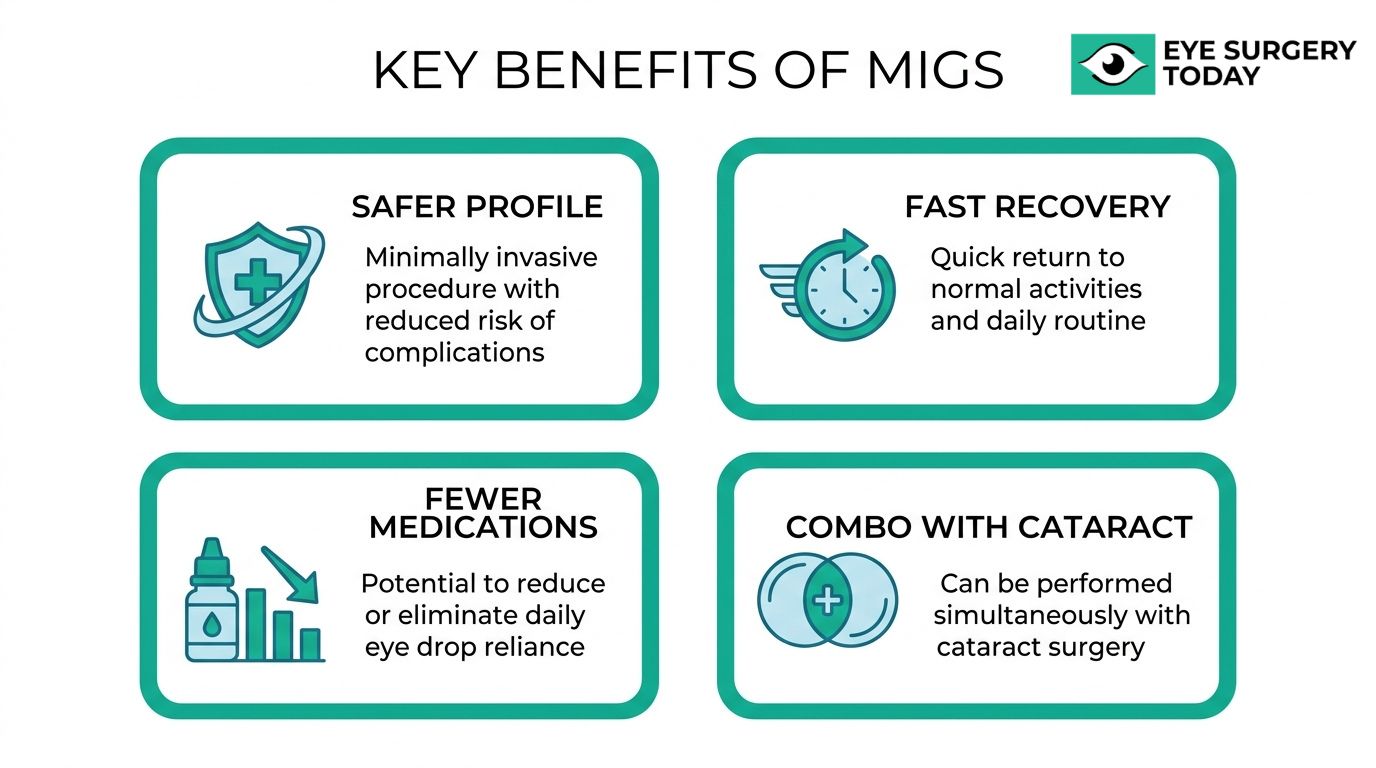
The potential benefits of MIGS include lower complication rates, faster recovery, reduced medication dependence, and the ability to combine the procedure with cataract surgery. These advantages make MIGS a consideration for patients with mild-to-moderate glaucoma who seek effective IOP reduction with less surgical risk than traditional approaches.
MIGS procedures can lower intraocular pressure to the mid-teens in many cases, while preserving conjunctival tissue for future surgical options if needed. According to a systematic review of 401 studies covering 39,381 eyes published between 2014 and 2024 in Clinical Ophthalmology, trabecular bypass implants showed lower rates of serious adverse events compared to suprachoroidal devices, and MIGS procedures generally lowered IOP to the mid-teens in mild-to-moderate primary open-angle glaucoma.
The key potential benefits of MIGS include:
- Favorable safety profile. MIGS uses an ab interno approach with minimal tissue trauma, which may reduce the risk of complications commonly associated with trabeculectomy or tube shunt procedures.
- Faster visual recovery. Postoperative recovery typically occurs within days to weeks, with vision stabilizing more rapidly compared to traditional glaucoma surgery.
- Reduced medication burden. Many patients experience a meaningful decrease in the number of glaucoma eye drops required after surgery, which can improve daily quality of life and long-term adherence.
- Compatibility with cataract surgery. MIGS procedures can often be performed during the same session as Local anesthesia, o, reducing overall surgical burden for patients who need both interventions.
- Preservation of future surgical options. Because MIGS causes minimal conjunctival and scleral disruption, patients retain the option of more aggressive filtration surgery later if their glaucoma progresses.
For many patients with mild-to-moderate disease, this combination of safety and efficacy represents one of the most practical reasons to discuss MIGS with an ophthalmologist early in the treatment process rather than waiting until the disease advances. Understanding the potential risks alongside these benefits helps patients make a fully informed decision.
What Are the Possible Risks and Complications of MIGS?
The possible risks and complications of MIGS include short-term side effects, other serious eye complications, and the chance that pressure reduction may be insufficient. The following subsections cover each category.
What Short-Term Side Effects May Occur After MIGS?
Short-term side effects that may occur after MIGS include mild, typically self-resolving issues during the first days to weeks of recovery. The most commonly reported early side effects are:
- Transient hyphema (small amounts of blood in the anterior chamber)
- Temporary eye pressure spikes in the immediate postoperative period
- Mild inflammation or irritation at the surgical site
- Blurred vision that usually stabilizes within days
- Light sensitivity during initial healing
According to a systematic review and meta-analysis of 875 eyes published by Dove Medical Press, the overall complication rate for MIGS (excluding transient self-resolving hyphema) was 16%, with sustained reduction in both intraocular pressure and medication burden. Most short-term side effects resolve without additional intervention, which is one reason MIGS carries a more favorable recovery profile than traditional filtration surgeries. Still, patients should report any sudden pain, significant vision loss, or worsening redness to their ophthalmologist promptly, as early evaluation can prevent minor issues from progressing.
What Rare but Serious Complications Should Patients Know?
Rare but serious complications that patients should know about include device malposition, persistent hypotony (abnormally low eye pressure), chronic inflammation, and, in exceptional cases, endophthalmitis. A systematic review of 401 studies covering 39,381 eyes published in Clinical Ophthalmology between 2014 and 2024 found that safety profiles vary across MIGS categories; trabecular bypass implants showed lower rates of serious adverse events compared to suprachoroidal devices.
Although these severe outcomes are uncommon, awareness helps set realistic expectations. Suprachoroidal and subconjunctival approaches, because they create drainage pathways outside the conventional route, may carry slightly elevated risk compared to trabecular-based procedures. For most candidates with mild-to-moderate glaucoma, the overall serious complication rate remains substantially lower than with trabeculectomy or tube shunt surgery. Your ophthalmologist can help weigh individual risk factors before selecting a specific procedure.
Can MIGS Fail to Lower Eye Pressure Enough?
Yes, MIGS can fail to lower eye pressure enough in some patients. Because MIGS procedures generally target a moderate IOP reduction, they may not achieve the aggressive pressure lowering that advanced or refractory glaucoma cases require. The American Academy of Ophthalmology Preferred Practice Guidelines state that a reasonable initial treatment goal for primary open-angle glaucoma is to reduce intraocular pressure by 20% to 30% below baseline; not every MIGS procedure reaches this threshold for every eye.
Factors that may contribute to an insufficient response include:
- Severity of trabecular meshwork damage or outflow resistance
- Scarring or fibrosis that develops around the device or drainage site
- Progression of glaucoma beyond the procedure’s intended scope
- Individual anatomical variation in outflow pathways
When MIGS does not produce adequate pressure control, your ophthalmologist may recommend additional medications, a repeat or different MIGS procedure, or escalation to traditional surgery such as trabeculectomy. Understanding these expectations before surgery helps patients and their care teams plan a long-term pressure management strategy.
How Much May MIGS Reduce the Need for Glaucoma Medications?
MIGS may reduce the need for glaucoma medications by lowering intraocular pressure enough that fewer daily eye drops are required to maintain target levels. The degree of medication reduction varies by procedure type, disease severity, and individual patient factors.
Many patients with mild-to-moderate open-angle glaucoma use one or more topical medications before surgery. When a MIGS procedure successfully lowers IOP, the treating ophthalmologist may be able to taper or eliminate some of those drops during follow-up visits. According to the American Academy of Ophthalmology Preferred Practice Guidelines, a reasonable initial treatment goal for primary open-angle glaucoma is to reduce intraocular pressure by 20% to 30% below baseline. Achieving this threshold through a MIGS procedure can shift the balance so that fewer medications, or sometimes none, are needed to stay within a safe pressure range.
Not every patient will become completely drop-free. Some may still require one medication where they previously used three, while others with well-controlled mild glaucoma may discontinue drops entirely. The realistic expectation, for most candidates, is a meaningful reduction in medication burden rather than guaranteed elimination. This practical benefit extends beyond convenience; fewer drops can mean fewer preservative-related side effects on the ocular surface, better long-term adherence, and improved quality of life. Discussing specific medication reduction goals with a glaucoma specialist before surgery helps set appropriate expectations for each individual case.
What Should You Expect Before, During, and After MIGS?
You should expect a streamlined process with brief preparation, a short procedure under local anesthesia, and a faster recovery compared to traditional glaucoma surgery. The following sections cover preparation steps, what occurs in the operating room, and the recovery timeline.
How Should You Prepare for a MIGS Procedure?
You should prepare for a MIGS procedure by working closely with your ophthalmologist to optimize your eye health in the weeks leading up to surgery. Preoperative steps typically include:
- Completing a comprehensive eye exam to confirm glaucoma severity and candidacy.
- Reviewing your current glaucoma medications with your surgeon, who may adjust your regimen before the procedure.
- Addressing any ocular surface issues, such as dry eye or inflammation, since a healthy corneal surface improves surgical precision.
- Arranging transportation home, as you will not be able to drive immediately after surgery.
- Following specific instructions about food, drink, and medication use the morning of the procedure.
Your surgeon may also discuss whether combining MIGS with cataract surgery makes sense for your situation, as this combined approach can reduce the need for a separate operation. Asking questions during this visit is essential; preparation is as much about understanding the process as it is about following clinical instructions.
What Happens During a MIGS Procedure?
A MIGS procedure happens through a tiny incision inside the eye, using an approach called ab interno. The surgeon accesses the eye’s drainage structures through the same small corneal entry point used in cataract surgery, which avoids external cuts to the conjunctiva or sclera. Local anesthesia, often with light sedation, keeps the patient comfortable throughout.
Using a specialized microscope and a goniolens for visualization, the surgeon implants a microstent, opens drainage tissue, or applies laser energy, depending on the specific device chosen. Most MIGS procedures take only 10 to 20 minutes when performed as a standalone operation. When combined with cataract surgery, the MIGS component adds only a few additional minutes to the overall time. Because tissue disruption is minimal, the eye remains structurally intact, which contributes directly to the favorable safety profile that distinguishes MIGS from traditional filtering surgeries.
What Does Recovery After MIGS Look Like?
Recovery after MIGS typically involves a shorter healing period than traditional glaucoma surgeries like trabeculectomy. Most patients notice vision stabilizing within days to weeks, and normal daily activities can often resume within a few days. Your ophthalmologist may prescribe anti-inflammatory or antibiotic eye drops for a limited period following the procedure. Understanding and adhering to post-operative instructions is crucial for proper healing and to prevent complications after eye surgery.
Common questions patients ask during recovery include how soon they can stop using glaucoma eye drops, what the expected timeline for pressure stabilization looks like, and how long-term outcomes compare to traditional surgeries. According to a report from Greenwich Eye, the most frequent patient inquiries about MIGS center on recovery time, the potential to discontinue eye drops, and how MIGS compares to trabeculectomy in terms of lasting success and safety.
Follow-up appointments in the first few weeks allow your surgeon to monitor intraocular pressure and healing. While some patients may eventually reduce their medication burden, this decision should always be guided by your eye care provider based on measured results. The recovery process and expected healing timeline are crucial discussions for any vision surgery, including procedures like eyelid surgery.
Understanding what to expect from recovery helps set realistic goals for the weeks ahead, especially when evaluating how MIGS compares to other glaucoma treatments.
How Does MIGS Compare to Other Glaucoma Treatments?
MIGS compares to other glaucoma treatments by offering a safer surgical profile with moderate IOP reduction, positioned between conservative options and more invasive procedures. The following subsections compare MIGS to eye drops, laser trabeculoplasty, and traditional surgeries.
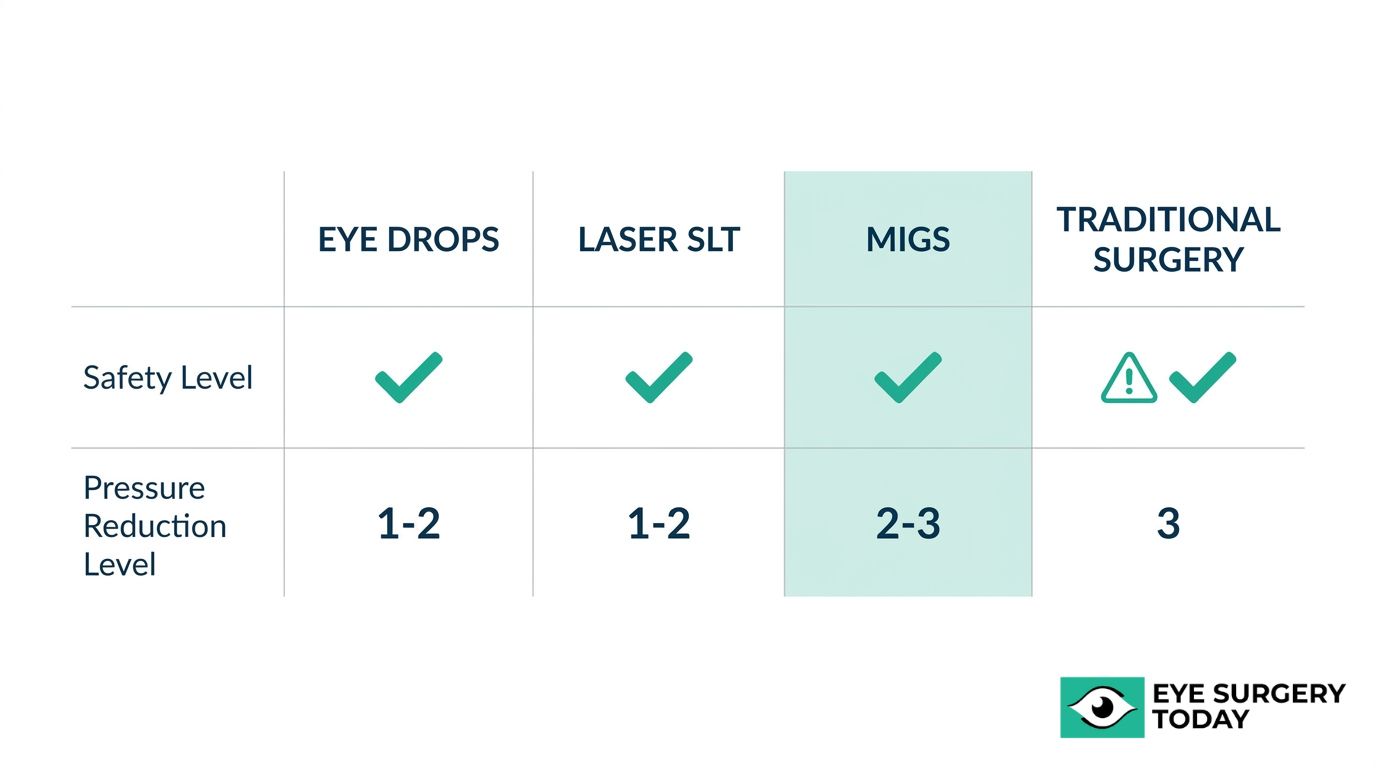
How Does MIGS Compare to Glaucoma Eye Drops?
MIGS compares to glaucoma eye drops by providing a surgical alternative that may reduce or eliminate daily medication burden while lowering intraocular pressure through a one-time procedure. Eye drops remain the most common first-line treatment, yet long-term adherence presents a significant challenge for many patients. Side effects from preservatives in topical medications, such as ocular surface irritation and dry eye, can worsen over time.
MIGS addresses these limitations by targeting the drainage pathway directly, often reducing the number of drops a patient needs. As Dr. Reay H. Brown, a board-certified ophthalmologist and glaucoma specialist, highlights, “the superior safety profile of MIGS compared to traditional filtering procedures has enabled earlier surgical intervention for glaucoma.”
For patients who struggle with consistent drop application or experience intolerable side effects, MIGS may offer a more sustainable approach to pressure management. However, some patients still require supplemental drops after a MIGS procedure, particularly those with higher baseline pressures.
How Does MIGS Compare to Laser Trabeculoplasty (SLT)?
MIGS compares to laser trabeculoplasty by offering a more sustained structural intervention, while SLT provides a noninvasive, repeatable option that may serve as an earlier step in the treatment ladder. SLT uses targeted laser energy to stimulate the trabecular meshwork and improve aqueous outflow without creating a permanent implant or incision.
According to research published in ScienceDirect, SLT can achieve intraocular pressure reduction comparable to topical medications at 6 to 12 months post-treatment, with a mean difference of only 0.04 mmHg. This makes SLT an effective initial option, though its effects can diminish over time.
MIGS procedures, by contrast, create a physical change to the drainage anatomy that may provide longer-lasting pressure reduction. The trade-off is that MIGS involves an operating room setting and carries slightly higher procedural risk than a laser performed in the office. For mild glaucoma, either approach can be appropriate; the choice often depends on disease progression and surgical candidacy.
How Does MIGS Compare to Trabeculectomy or Tube Shunts?
MIGS compares to trabeculectomy and tube shunts by offering a significantly safer risk profile at the cost of less aggressive IOP reduction. Trabeculectomy creates a scleral flap and removes trabecular tissue to form a subconjunctival bleb for drainage. Tube shunts use a silicone tube placed in the anterior chamber to divert aqueous humor to an external plate on the sclera. Both procedures can achieve lower target pressures than most MIGS devices.
However, these traditional surgeries carry higher rates of serious complications, such as hypotony, bleb-related infections, and prolonged recovery. MIGS procedures generally produce faster visual recovery, less tissue disruption, and fewer sight-threatening adverse events.
- Trabeculectomy and tube shunts may be more appropriate for advanced or refractory glaucoma requiring aggressive IOP targets.
- MIGS is often better suited for mild-to-moderate disease where a moderate pressure reduction meets treatment goals.
- Traditional surgeries typically require more intensive postoperative monitoring and longer recovery periods.
For most patients with early to moderate disease, MIGS represents a practical balance between meaningful pressure reduction and surgical safety. When glaucoma progresses beyond what MIGS can manage, trabeculectomy or tube shunts remain important options in the treatment algorithm.
How Do You Choose the Right MIGS Procedure for Your Eyes?
You choose the right MIGS procedure for your eyes by working with a glaucoma specialist who evaluates your disease severity, eye anatomy, medication burden, and surgical goals.
What Factors Does Your Ophthalmologist Consider When Recommending MIGS?
Your ophthalmologist considers several key factors when recommending MIGS:
- Glaucoma stage and type: Mild-to-moderate open-angle glaucoma may respond well to trabecular bypass devices, while more advanced cases might require canal-based or subconjunctival approaches.
- Target IOP range: The specific pressure reduction needed influences which drainage pathway the surgeon targets.
- Current medication burden: Patients on multiple drops who struggle with adherence may benefit from procedures with stronger medication-reducing profiles.
- Lens status and cataract plans: Many MIGS procedures are combined with cataract surgery, which affects both timing and device selection.
- Ocular anatomy: Angle structure, prior surgeries, and conjunctival health all shape which approach is safest.
According to a Review of Optometry report, postoperative recovery for MIGS typically occurs within days to weeks, with vision stabilizing rapidly compared to traditional surgery. This quick recovery timeline can itself become a deciding factor for patients balancing work and daily responsibilities.
Why Is a Personalized Evaluation Essential Before MIGS?
A personalized evaluation is essential before MIGS because no single procedure works best for every patient. Glaucoma varies widely in its mechanism, progression rate, and response to treatment. Two patients with the same IOP reading may have very different angle anatomy, optic nerve damage patterns, and medication tolerances.
A thorough preoperative assessment typically includes gonioscopy to visualize the drainage angle, optical coherence tomography to assess nerve fiber layer health, and a complete review of the patient’s medication history. These findings help the surgeon match the procedure’s drainage mechanism to the patient’s specific anatomy and treatment goals.
For most patients with mild-to-moderate disease, the decision often comes down to which outflow pathway offers the best balance of pressure reduction and safety for their individual case. Rushing this evaluation risks selecting a procedure that underperforms or introduces unnecessary risk.
Understanding what goes into this decision puts patients in a stronger position to have informed conversations with their eye care team. Such comprehensive assessments are critical for all types of vision correction, including procedures like LASIK for refractive errors, ensuring optimal outcomes and patient satisfaction across different surgical specialties.
How Can Surgeon-Reviewed Resources Help You Understand MIGS?
Surgeon-reviewed resources can help you understand MIGS by providing clinically accurate, accessible information vetted by practicing ophthalmologists. The following subsections cover how Eye Surgery Today supports MIGS education and the key takeaways from this overview.
Can Eye Surgery Today Help You Learn About MIGS and Related Procedures?
Yes, Eye Surgery Today can help you learn about MIGS and related procedures through its surgeon-reviewed educational platform. Every article, guide, and resource on the site is reviewed by nationally recognized ophthalmologists who bring real-world clinical experience to each topic. This review process ensures the information reflects current evidence-based practice while remaining free of unnecessary medical jargon.
Eye Surgery Today covers a broad range of eye surgery topics, including:
- Cataract surgery fundamentals and advanced intraocular lens options
- Glaucoma treatment approaches, including MIGS procedures
- Recovery expectations and safety profiles for various procedures
- Decision-making guides that help patients compare treatment options
The platform was built to bridge the gap between complex surgical knowledge and everyday patient understanding. Rather than replacing a conversation with your eye doctor, these resources prepare you to ask better questions and feel more confident during consultations. For patients exploring whether MIGS may be appropriate for their glaucoma, having access to unbiased, surgeon-reviewed content can make a meaningful difference in how they approach treatment decisions.
What Are the Key Takeaways About MIGS Options and Overview?
The key takeaways about MIGS options and overview center on safety, versatility, and suitability for mild-to-moderate glaucoma. MIGS procedures use an ab interno approach with minimal tissue disruption, offering a favorable safety profile compared to traditional filtration surgeries.
Core points to remember include:
- Multiple MIGS categories exist, such as trabecular bypass microstents, canal-based procedures, suprachoroidal shunts, subconjunctival filtering devices, and aqueous suppression with ECP.
- Each procedure targets a different outflow pathway, so the right choice depends on glaucoma severity, anatomy, and whether cataract surgery is planned.
- MIGS may help reduce dependence on daily glaucoma eye drops, though results vary by procedure and patient.
- Candidacy typically favors patients with ocular hypertension or mild-to-moderate open-angle glaucoma, while advanced cases may still require traditional surgery.
- Recovery after MIGS is generally faster than after trabeculectomy or tube shunt placement.
No single MIGS procedure is ideal for every patient. Discussing your specific diagnosis, treatment goals, and lifestyle preferences with a qualified glaucoma specialist remains the most reliable path to choosing the right approach. Surgeon-reviewed resources like those on Eye Surgery Today can help you prepare for that conversation with confidence.





