IOL exchange is a surgical procedure that removes a previously implanted intraocular lens after cataract surgery and replaces it with a new one to address visual problems such as incorrect lens power, lens dislocation, or dissatisfaction with the original implant’s optical performance.
This guide covers the surgical process and timing of IOL exchange, the clinical reasons it may be recommended, candidacy and replacement lens options, how it compares to alternative corrections, potential risks, and what to expect during recovery.
The procedure involves freeing the original lens through viscodissection, refolding it for safe removal through a small corneal incision, and implanting a replacement lens matched to updated measurements. When performed within the first several months, the capsular bag remains pliable enough for straightforward extraction; longer delays can introduce fibrosis that complicates removal and may require alternative fixation methods like scleral or iris attachment.
Common indications include significant refractive error from an incorrect IOL power, multifocal lens dissatisfaction related to neuroadaptation difficulty or persistent glare, and lens dislocation caused by weakened capsular support. Conditions such as new retinal disease or the need for future vitreoretinal surgery may also prompt a lens change.
Replacement options span monofocal, multifocal, trifocal, extended depth of focus, and toric designs, each selected based on the patient’s anatomy and visual priorities. Compared to piggyback implantation or LASIK enhancement, IOL exchange is the only option that fully addresses lens-related problems rather than compensating around them.
Recognized complications include cystoid macular edema, retinal detachment, corneal edema, infection, and elevated eye pressure. Recovery generally takes four to six weeks, with vision stabilizing gradually over that period.
What Happens During an IOL Exchange Procedure?
An IOL exchange procedure involves removing the original intraocular lens and implanting a new replacement lens through a small corneal incision. The following sections cover lens removal, implantation, and surgical duration.
How Is the Original Intraocular Lens Removed?
The original intraocular lens is removed through a careful, stepwise process designed to protect surrounding eye structures. The surgeon begins by creating a small incision in the cornea, then injects a viscoelastic substance behind the IOL to gently separate it from the capsular bag, a technique known as viscodissection.
Once freed, the lens must be brought into the anterior chamber for extraction. Because most modern IOLs are foldable acrylic, the surgeon can refold the lens within the anterior chamber before withdrawing it through the incision. This approach, sometimes called the “twist and out” technique, minimizes contact with the corneal endothelium and reduces the risk of corneal cell damage.
In cases where the IOL has become firmly adhered to the capsular bag over time, removal grows more complex. Scar tissue and fibrosis may require additional dissection, which is one reason timing matters in IOL exchange decisions.
How Is the New Replacement Lens Implanted?
The new replacement lens is implanted immediately after the original IOL is removed, using the same corneal incision whenever possible. The surgeon selects a replacement lens based on updated biometry measurements and the patient’s visual goals.
If the capsular bag remains intact and stable, the new IOL is placed directly into it. This position offers the most predictable refractive outcomes and long-term stability. When capsular support is insufficient, alternative fixation methods become necessary:
- An anterior chamber IOL can be placed in front of the iris.
- An iris-fixated posterior chamber IOL attaches directly to the iris for support.
- Scleral-fixation techniques, such as the Yamane method, secure the haptics within the scleral wall.
Each fixation approach carries its own risk-benefit profile, so the surgeon’s choice depends on the individual anatomy encountered during surgery. For most patients undergoing a straightforward exchange, capsular bag placement remains the preferred option.
How Long Does an IOL Exchange Surgery Take?
IOL exchange surgery typically takes 30 to 60 minutes, though duration varies based on the complexity of lens removal and the fixation method required. Cases involving a well-preserved capsular bag tend to be shorter, while those requiring scleral fixation or management of fibrosis may extend the surgical time.
Despite its complexity, outcomes are generally favorable. According to a retrospective study published in Clinical Ophthalmology, IOL exchange significantly improved mean uncorrected visual acuity from 20/192 preoperatively to 20/61 at last follow-up, with 78.7% of eyes achieving a refractive outcome within ±1.0 diopter of the target.
These results underscore that while the procedure demands more surgical skill than initial cataract surgery, it can meaningfully restore functional vision when performed by an experienced surgeon. Understanding the expected recovery timeline and potential risks helps patients set realistic expectations before proceeding.
Why Would Someone Need an IOL Exchange After Cataract Surgery?
Someone may need an IOL exchange after cataract surgery due to incorrect lens power, multifocal IOL dissatisfaction, lens dislocation, persistent visual disturbances, or incompatibility with a new eye condition. Each scenario presents distinct challenges.
What If the IOL Power Is Incorrect and Vision Is Blurry?
An incorrect IOL power can leave vision blurry because the implanted lens does not match the eye’s actual refractive needs. Biometry measurement errors, unusual corneal curvature, or prior refractive surgery history may contribute to this mismatch. According to a review published in Clinical Ophthalmology, the most frequent indications for IOL exchange include incorrect IOL power, IOL dislocation, uveitis-glaucoma-hyphema syndrome, and patient dissatisfaction due to refractive outcomes or visual disturbances.
When the refractive error is significant enough that glasses or contact lenses cannot adequately compensate, exchanging the lens for one with the correct dioptric power may be recommended by the surgeon. Minor power discrepancies, however, can sometimes be addressed through less invasive options before exchange becomes necessary.
What If the Patient Is Unhappy With a Multifocal IOL?
Patient unhappiness with a multifocal IOL is one of the more common reasons for considering an exchange. Blurred vision is the leading cause of dissatisfaction among patients with multifocal IOLs, often occurring without a clear organic explanation such as retinal disease or residual refractive error. Neuroadaptation failure, where the brain struggles to adjust to the lens’s split-focus optics, can make everyday tasks frustrating.
According to a study published in Eye and Vision, dissatisfaction following multifocal IOL implantation can be successfully managed in approximately 80% of cases by exchanging the lens with a different multifocal IOL optical profile. In some cases, switching to a monofocal or extended depth of focus lens may better suit the patient’s visual priorities and lifestyle.
What If the IOL Has Dislocated or Shifted Out of Position?
An IOL that has dislocated or shifted out of position can cause sudden blurred vision, double images, or visible lens edge effects. Dislocation may occur when the capsular bag weakens over time, particularly in patients with pseudoexfoliation syndrome or a history of ocular trauma. Zonular fiber deterioration, which naturally progresses with age, can also allow the lens to decenter or drop.
A partially displaced IOL sometimes causes intermittent symptoms that worsen with head movement or changes in gaze. Complete dislocation into the vitreous cavity typically requires surgical intervention. Your ophthalmologist may recommend IOL exchange with a scleral-fixated or iris-fixated replacement lens when capsular support is no longer adequate to hold the original implant.
What If There Is Persistent Glare or Halos After Surgery?
Persistent glare or halos after cataract surgery may result from the IOL’s optical design interacting unfavorably with the patient’s pupil size or corneal characteristics. Diffractive multifocal lenses, in particular, split incoming light into multiple focal points, which can produce noticeable rings around light sources at night.
While mild halos often diminish as the brain adapts over several months, symptoms that remain severe and interfere with driving or daily activities may warrant intervention. An ophthalmologist may recommend exchanging the lens for a monofocal or extended depth of focus IOL that produces fewer photic disturbances. This decision is typically made only after confirming that other causes, such as posterior capsule opacification or dry eye, have been ruled out.
What If the IOL Is Incompatible With a New Eye Condition?
An IOL may become incompatible with a new eye condition that develops after the original cataract surgery. Conditions such as macular degeneration, diabetic retinopathy, or epiretinal membrane can change the eye’s optical needs or make certain lens designs problematic. A multifocal IOL, for example, may reduce contrast sensitivity in ways that compound the visual challenges of retinal disease.
Silicone IOLs can also create complications if the patient later requires vitreoretinal surgery involving silicone oil tamponade, since the oil adheres to the lens surface and obscures vision. In these situations, your ophthalmologist may recommend exchanging the IOL for a design that better accommodates the evolving clinical picture, ensuring the replacement lens supports both current and anticipated treatment needs.
Understanding what drives the need for an exchange helps clarify the next critical question: timing.
When Is the Best Timing for an IOL Exchange?
The best timing for an IOL exchange depends on how well the eye has healed and the specific reason for the procedure. The sections below cover early and delayed timing considerations.
How Soon After Cataract Surgery Can an IOL Exchange Be Done?
An IOL exchange can be done as early as a few weeks after cataract surgery, though most ophthalmologists prefer to wait until the eye has fully stabilized. Recovery from cataract surgery usually takes four to six weeks, with vision improving gradually during this period, according to ReFocus Eye Health. Many patients find that visual acuity continues to adjust over several months.
Performing the exchange within the first few months offers a practical advantage: the capsular bag remains soft and pliable, making lens removal technically simpler. Surgeons can more easily separate the IOL from surrounding tissue before significant fibrosis develops. However, operating too early, before refractive measurements stabilize, may compromise the accuracy of the replacement lens power.
For most patients, the window between two to three months after the original cataract surgery balances healing completion with favorable surgical conditions. Your ophthalmologist may recommend waiting longer if inflammation persists or if the cornea needs additional recovery time.
What Happens If the IOL Exchange Is Delayed Too Long?
If the IOL exchange is delayed too long, the procedure becomes significantly more complex and carries higher surgical risk. Over time, the capsular bag contracts and fibrotic adhesions form between the IOL haptics and surrounding tissue. These changes make lens removal more difficult, sometimes requiring additional maneuvers that increase the chance of capsular rupture.
In a study published in Clinical Ophthalmology, IOL exchange occurred at a mean interval of 44.9 months after initial implantation in cases involving hydrophilic acrylic lens opacification. At such late stages, surgeons may encounter denser scar tissue that demands more aggressive dissection techniques.
Prolonged delays can also affect the range of replacement options available. If capsular support is lost during a complicated explantation, the new IOL may need scleral fixation or anterior chamber placement rather than standard in-the-bag positioning. These alternative fixation methods, while effective, introduce additional variables that would not apply in an earlier exchange.
In clinical practice, addressing known IOL problems sooner rather than later almost always results in a smoother procedure and more predictable visual outcome. With timing established, candidacy factors further determine whether an IOL exchange is the right path forward.
Who Is a Good Candidate for IOL Exchange?
A good candidate for IOL exchange is typically someone experiencing persistent visual problems after cataract surgery that cannot be resolved with simpler interventions. Eligibility depends on overall eye health and specific clinical factors.
What Eye Health Conditions May Affect IOL Exchange Eligibility?
Eye health conditions that may affect IOL exchange eligibility include corneal disease, glaucoma, retinal disorders, and chronic ocular inflammation. Each of these can increase surgical risk or limit the potential for visual improvement after the procedure.
Conditions that may influence candidacy include:
- Corneal endothelial dysfunction: Low endothelial cell counts may raise the risk of corneal edema during lens manipulation.
- Advanced glaucoma: Elevated baseline intraocular pressure or optic nerve damage can complicate postoperative recovery.
- Retinal pathology: Macular degeneration, diabetic retinopathy, or epiretinal membranes may limit the visual gains achievable through lens exchange.
- Chronic uveitis: Ongoing intraocular inflammation can worsen after additional surgical intervention.
- Insufficient capsular support: When the capsular bag is compromised, alternative fixation methods such as scleral fixation or iris fixation become necessary, adding complexity.
Patients with well-controlled versions of these conditions may still qualify, but thorough preoperative evaluation is essential. In practice, the patients who benefit most are those whose visual complaints trace directly to the IOL itself rather than to underlying ocular disease.
When Might a Surgeon Recommend Against IOL Exchange?
A surgeon might recommend against IOL exchange when the surgical risks outweigh the expected visual benefit, or when the patient’s symptoms can be addressed through less invasive means. This decision reflects a careful risk-benefit analysis rather than a blanket rule.
Situations where a surgeon may advise against the procedure include:
- Adequate alternative corrections: If LASIK enhancement or a piggyback lens can resolve the refractive error with lower risk.
- Significant endothelial compromise: Surgical techniques require careful manipulation near the cornea. According to ESCRS EuroTimes, expert recommendations emphasize techniques such as viscodissection and the “twist and out” method specifically to protect the endothelium during lens removal.
- High infection risk: Patients with a history of postoperative infection or those requiring concurrent anterior vitrectomy face elevated risk, since combined procedures carry a higher complication profile.
- Unrealistic visual expectations: When the source of dissatisfaction is unrelated to the IOL, such as pre-existing retinal disease or dry eye, exchanging the lens is unlikely to resolve symptoms.
Every candidacy decision ultimately rests on individualized clinical judgment. Understanding both eligibility factors and contraindications helps patients have more productive conversations with their ophthalmologist.
What Types of Replacement Lenses Can Be Used in an IOL Exchange?
The types of replacement lenses that can be used in an IOL exchange include monofocal, multifocal or trifocal, extended depth of focus, and toric IOLs. Each lens type addresses different visual needs.
Monofocal IOL
A monofocal IOL is a single-focus intraocular lens that provides clear vision at one set distance. Most patients choose monofocal lenses optimized for distance vision and rely on reading glasses for near tasks. Because monofocal IOLs deliver sharp optics at a fixed focal point, they may produce fewer visual disturbances, such as halos or glare, compared to multifocal designs. This predictability makes them a common choice when a patient exchanges a premium lens that caused intolerable side effects. For patients whose primary complaint is optical quality rather than spectacle dependence, a monofocal replacement often represents the most straightforward path to comfortable vision.
Multifocal or Trifocal IOL
A multifocal or trifocal IOL is a lens designed to provide clear vision at multiple distances, reducing dependence on glasses for both near and far tasks. Trifocal designs add an intermediate focal point for activities like computer work. These lenses split incoming light into distinct zones, which can introduce halos or glare in some patients. Successful neuroadaptation is essential; the brain must learn to select the appropriate focal image. When an IOL exchange involves replacing one multifocal with another, selecting a different optical profile can resolve prior complaints. In clinical practice, switching the diffractive pattern or ring spacing often addresses the specific visual disturbance that prompted dissatisfaction with the original lens.
Extended Depth of Focus IOL
An extended depth of focus IOL is a lens that elongates a single focal point rather than splitting light into separate zones. This design creates a continuous range of vision from distance through intermediate without the sharp optical transitions found in multifocal lenses. As a result, extended depth of focus IOLs may produce fewer halos and less glare, making them well suited for patients who experienced these symptoms with a prior multifocal implant. Near vision, however, may still require reading glasses for fine print. For patients who value smooth visual transitions and nighttime driving comfort, this lens category often strikes an effective balance between functional range and optical clarity.
Toric IOL for Astigmatism
A toric IOL is a lens engineered to correct astigmatism by incorporating different optical powers along specific meridians. Precise rotational alignment during implantation is critical; even small degrees of misalignment can reduce the astigmatism-correcting benefit. When residual or uncorrected astigmatism is the reason for an IOL exchange, replacing the original lens with a toric design directly addresses the cylindrical refractive error. Toric models are available in monofocal, multifocal, and extended depth of focus configurations, allowing surgeons to correct astigmatism while simultaneously matching the patient’s desired focal range. This versatility makes toric IOLs one of the most practical options in lens selection.
Understanding which replacement lens best fits your visual goals helps guide the next step: weighing IOL exchange against other corrective options.
How Does IOL Exchange Compare to Other Corrective Options?
IOL exchange compares to other corrective options by offering a complete lens replacement, while alternatives like piggyback implantation or LASIK enhancement correct vision without removing the existing IOL.
How Does IOL Exchange Compare to Piggyback Lens Implantation?
IOL exchange compares to piggyback lens implantation in both surgical approach and refractive predictability. IOL exchange, also called lens replacement surgery or IOL explantation and reimplantation, removes the original intraocular lens entirely and replaces it. Piggyback lens implantation places a secondary lens on top of the existing IOL without removing it, making it a less invasive option.
According to a comparative study published in the Journal of Refractive Surgery, predictability within ±1.0 diopter of the refractive target was achieved in 62.5% of eyes undergoing IOL exchange compared to 85% for piggyback lens implantation. This difference suggests that when residual refractive error is the primary concern, a piggyback approach may offer more precise correction with fewer surgical risks. However, piggyback lenses cannot address problems like IOL opacification, dislocation, or optical design dissatisfaction, where full exchange remains the only viable solution.
For surgeons weighing these options, the clinical indication often dictates the choice more than predictability data alone.
How Does IOL Exchange Compare to LASIK Enhancement?
IOL exchange compares to LASIK enhancement by addressing fundamentally different layers of the visual system. LASIK enhancement reshapes the cornea to correct residual refractive error after cataract surgery, while IOL exchange replaces the intraocular lens itself. When the issue is purely a minor spherical or cylindrical error, LASIK offers a less invasive correction with potentially higher precision. In the same comparative study from the Journal of Refractive Surgery, LASIK achieved 100% predictability within ±1.0 diopter of target, outperforming both IOL exchange and piggyback implantation for refractive accuracy.
LASIK enhancement, though, cannot resolve problems originating from the lens itself, such as:
- IOL dislocation or subluxation
- Unwanted optical side effects from a multifocal IOL design
- Lens opacification or material degradation
Corneal thickness and health must also be sufficient for LASIK to be a safe option. For purely refractive fine-tuning, LASIK enhancement is often the most predictable path; for lens-related complications, IOL exchange remains necessary.
Understanding how these options compare can help clarify the potential risks involved with each approach.
What Are the Possible Risks and Complications of IOL Exchange?
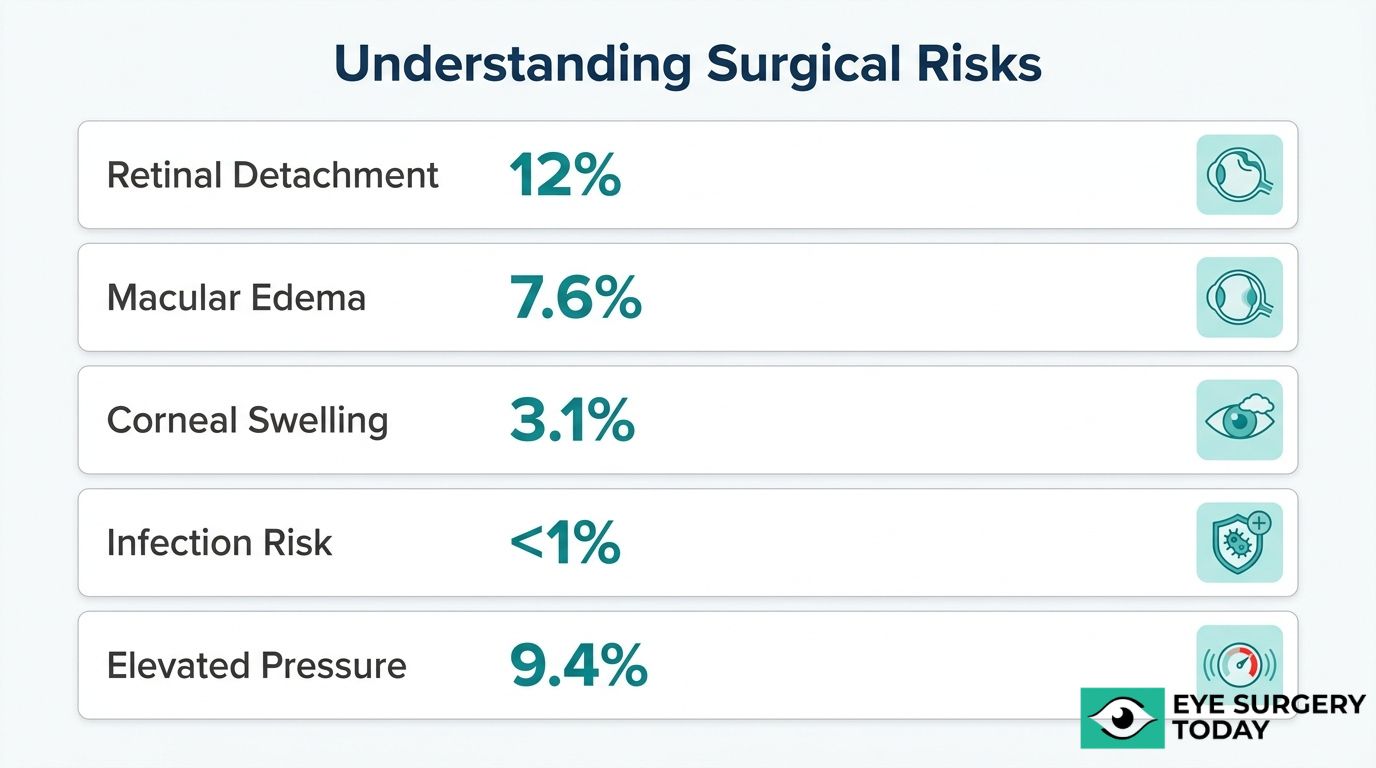
The possible risks and complications of IOL exchange include retinal detachment, corneal edema, cystoid macular edema, infection, and elevated eye pressure. The following subsections cover each complication in detail.
What Is the Risk of Retinal Detachment During IOL Exchange?
The risk of retinal detachment during IOL exchange is significant, even in eyes without pre-existing risk factors. According to a long-term follow-up study published in Clinical Ophthalmology, 12% of eyes developed a retinal detachment following IOL exchange, identifying it as a serious sight-threatening complication even in eyes without predisposing ocular comorbidities.
This rate makes retinal detachment one of the more concerning outcomes associated with secondary lens procedures. Because the vitreous and retina can be disturbed during lens removal and reimplantation, the mechanical forces involved may contribute to retinal tears that progress to detachment over time. Patients with high myopia or prior vitreoretinal issues may face elevated baseline risk, which is why thorough preoperative retinal evaluation is essential before proceeding.
Can IOL Exchange Cause Corneal Edema or Damage?
Yes, IOL exchange can cause corneal edema or damage due to intraoperative manipulation near the corneal endothelium. Removing the original lens and inserting a replacement requires instruments to pass through or near the anterior chamber, which places endothelial cells at risk of mechanical trauma.
A related concern is cystoid macular edema (CME), which was identified as the most frequent complication following IOL exchange. A large retrospective study published in Clinical Ophthalmology found CME occurring in 7.6% of cases. While corneal edema typically resolves within days to weeks with anti-inflammatory treatment, CME can persist longer and may require targeted therapy. Surgeons often use protective viscoelastic agents during the procedure to minimize endothelial cell loss, though some degree of corneal stress remains inherent to the surgery.
What Is the Risk of Infection After IOL Exchange?
The risk of infection after IOL exchange is low but clinically meaningful. Postoperative endophthalmitis, the most serious infectious complication, occurs at a higher rate in secondary IOL procedures compared to primary cataract surgery. According to a report from Review of Ophthalmology, the 42-day postoperative endophthalmitis rate for IOL exchange was 0.28% overall, increasing to 0.42% when the procedure was combined with an anterior vitrectomy.
Although these percentages appear small, endophthalmitis can cause severe, irreversible vision loss without prompt treatment. Prophylactic intracameral antibiotics administered at the time of surgery remain one of the most effective preventive strategies. Strict sterile technique and careful postoperative monitoring further reduce the likelihood of this complication.
How Common Is Elevated Eye Pressure After the Procedure?
Elevated eye pressure after IOL exchange is a recognized postoperative complication, though it is often transient. Intraocular pressure (IOP) spikes can occur in the hours or days following surgery due to retained viscoelastic material, inflammatory debris, or changes in aqueous humor dynamics caused by the new lens position.
Most pressure elevations respond well to topical anti-glaucoma drops and resolve within the first week. However, patients with a history of glaucoma or ocular hypertension may experience more persistent IOP changes requiring extended monitoring. In rare cases involving scleral-fixated or anterior chamber IOLs, chronic pressure elevation can develop if the lens physically obstructs drainage structures. Regular postoperative tonometry helps detect and manage IOP changes before they cause optic nerve damage.
With these risks understood, knowing what to expect during recovery helps patients prepare for the healing process ahead.
What Should You Expect During IOL Exchange Recovery?
You should expect a gradual healing process that unfolds over several weeks. The subsections below cover recovery timelines, normal early vision changes, and the follow-up schedule your ophthalmologist may recommend.
How Long Does It Take to Recover From an IOL Exchange?
Recovery from an IOL exchange typically takes four to six weeks, with vision improving gradually during this period. According to ReFocus Eye Health, many patients find that vision continues to adjust over several months even after the initial healing window closes.
The first week tends to involve the most noticeable discomfort, including mild soreness, light sensitivity, and watery eyes. Most ophthalmologists prescribe anti-inflammatory and antibiotic eye drops during this phase to manage swelling and reduce infection risk. By weeks two through four, inflammation usually subsides and visual clarity begins to stabilize. Patients who received a multifocal or extended depth of focus replacement lens may need additional time for neuroadaptation, as the brain adjusts to processing images through the new optic.
Returning to light daily activities is often possible within a few days, though strenuous exercise and heavy lifting are generally restricted for several weeks. This focus on post-operative care and activity restrictions is crucial for healing, similar to the recovery protocols for other ophthalmic procedures like eyelid surgery. Patients who closely follow their postoperative drop schedule and activity restrictions tend to reach stable vision faster and with fewer setbacks.
What Vision Changes Are Normal in the First Weeks?
The vision changes that are normal in the first weeks include mild blurriness, fluctuating clarity, and increased sensitivity to light. These symptoms reflect the eye’s inflammatory response and the gradual stabilization of the replacement lens inside the eye.
During the first few days, vision may seem hazy or washed out as residual surgical swelling affects the cornea and surrounding tissues. Slight fluctuations in sharpness throughout the day are common, particularly in the morning when fluid shifts overnight can temporarily alter how light passes through the eye. Some patients also notice:
- Mild glare or halos around lights, especially at night
- A slight difference in color perception between the operated and non-operated eye
- Occasional dry eye sensations that affect visual comfort
These changes typically diminish steadily over two to four weeks. If vision suddenly worsens, new floaters appear, or sharp pain develops, contacting your ophthalmologist promptly is essential, as these could signal complications such as elevated eye pressure or early retinal changes.
What Follow-Up Appointments Are Needed After IOL Exchange?
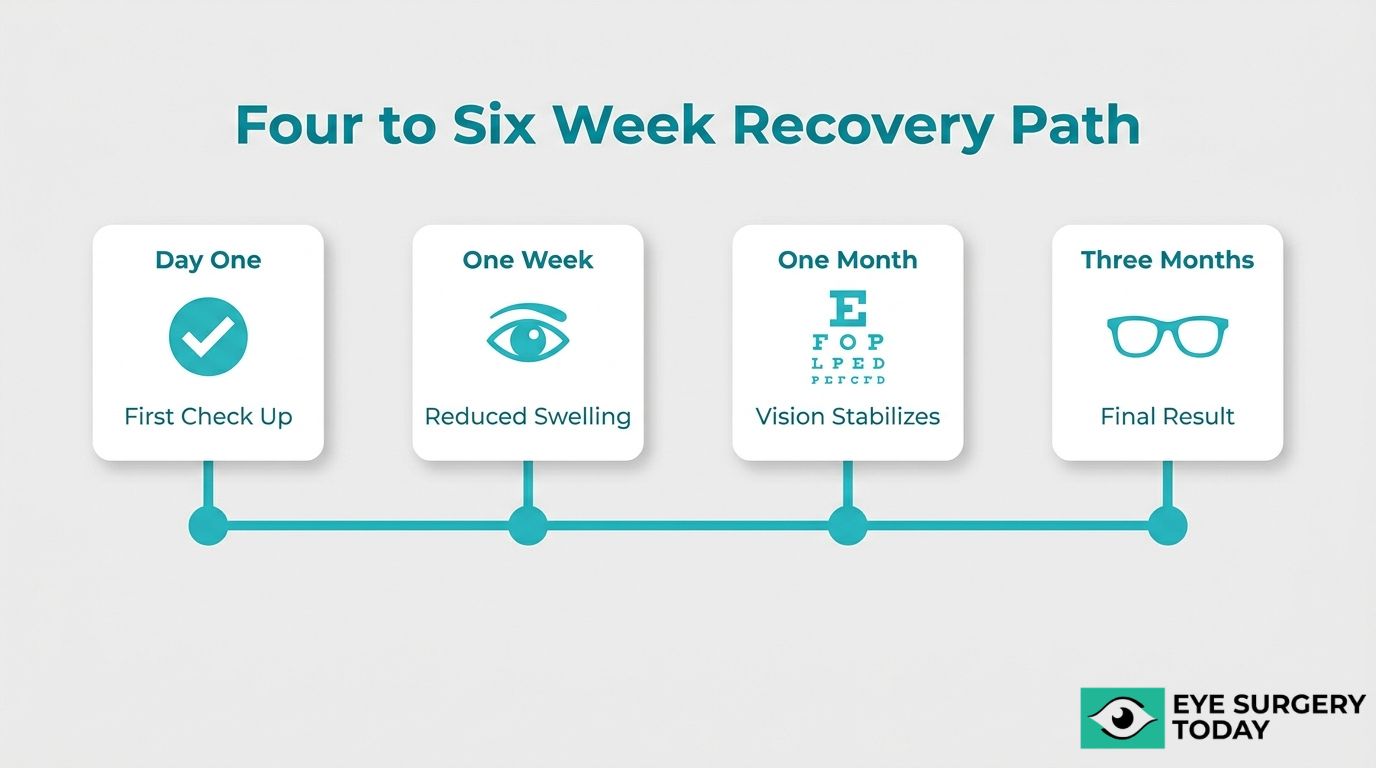
The follow-up appointments needed after IOL exchange generally include visits at one day, one week, one month, and three months postoperatively. Your ophthalmologist may adjust this schedule based on individual healing and any complications observed during earlier visits.
The day-one check focuses on confirming proper lens positioning, measuring eye pressure, and ruling out early signs of infection. At the one-week appointment, your surgeon evaluates inflammation levels and adjusts drop medications if needed. The one-month visit typically includes a refraction assessment to determine how the new lens is performing against the target prescription.
By the three-month mark, most patients have reached stable vision, making this an appropriate time for a final refractive measurement and updated eyeglass prescription if necessary. Patients with scleral-fixated or iris-fixated lenses may require additional monitoring visits, since these fixation methods carry a slightly higher risk of late lens tilt or displacement.
Consistent attendance at each scheduled visit gives your surgeon the best opportunity to detect and address any issue early, contributing to ongoing eye wellness and keeping your recovery on track toward the best possible visual outcome.
How Successful Is IOL Exchange at Improving Vision Outcomes?
IOL exchange is successful at improving vision outcomes for the majority of patients, though results vary by indication and surgical approach. The following details cover visual acuity improvements, refractive predictability, and how success compares across corrective alternatives.
In one case, IOL exchange surgery significantly improved mean uncorrected visual acuity from 20/192 preoperatively to 20/61 at last follow-up, according to a retrospective study published in Clinical Ophthalmology. That same analysis found 78.7% of eyes achieved a refractive outcome within ±1.0 diopter of the target refraction.
For patients with multifocal IOL dissatisfaction, outcomes can be equally encouraging. When the exchange involves switching to a different multifocal optical profile, approximately 80% of cases result in successful management of visual complaints related to neuroadaptation failure or poor quality of vision.
These numbers reflect meaningful improvement, but they also underscore an important clinical reality: IOL exchange delivers strong results when the underlying cause of dissatisfaction is correctly identified and the replacement lens is carefully matched to the patient’s visual needs. Refractive predictability, while good, does not reach the near-perfect precision of alternatives like LASIK for isolated refractive correction. For patients whose primary issue is lens-related, however, exchanging the IOL remains one of the most direct and effective solutions available.
Understanding success rates in context helps set realistic expectations before surgery, a topic your ophthalmologist can address when evaluating whether IOL exchange is the right path forward.
How Can Surgeon-Reviewed Guidance Help You Navigate an IOL Exchange Decision?
Surgeon-reviewed guidance can help you navigate an IOL exchange decision by providing expert evaluation of your specific visual complaints, candidacy factors, and replacement lens options. The sections below cover how Eye Surgery Today supports informed decision-making and the key takeaways about IOL exchange.
Can Eye Surgery Today Help You Understand Your IOL Options?
Yes, Eye Surgery Today can help you understand your IOL options through educational resources designed to clarify every aspect of lens replacement surgery. Eye Surgery Today is a physician-led education platform founded by nationally recognized key leaders in ophthalmology. The platform translates complex clinical information about intraocular lens choices, including monofocal, multifocal, toric, and extended depth of focus designs, into clear, accessible guidance.
Because IOL exchange involves weighing factors like capsular support, refractive targets, and lifestyle needs, having access to unbiased, expert-reviewed content can make the difference between confusion and confidence. Eye Surgery Today empowers patients to ask better questions during surgical consultations and approach their IOL exchange decision with a stronger understanding of what each lens type offers.
What Are the Key Takeaways About How IOL Exchange Works?
The key takeaways about how IOL exchange works center on understanding the procedure’s indications, timing, risks, and expected outcomes:
- IOL exchange removes a previously implanted intraocular lens and replaces it with a new one to correct issues such as incorrect lens power, IOL dislocation, persistent visual disturbances, or patient dissatisfaction with multifocal optics.
- Timing matters significantly; earlier exchanges generally involve less surgical complexity, while delayed procedures may require advanced fixation techniques if capsular support has deteriorated.
- Replacement lens selection depends on individual anatomy, visual goals, and whether adequate capsular bag support remains.
- Risks include cystoid macular edema, retinal detachment, corneal edema, infection, and elevated eye pressure, making thorough preoperative evaluation essential.
- Visual outcomes are favorable for most patients, though predictability can vary compared to alternatives like piggyback lens implantation or LASIK enhancement.
Every IOL exchange decision benefits from a detailed conversation with an experienced surgeon who can assess your unique ocular anatomy, weigh the procedural risks against expected visual gains, and recommend the most appropriate lens for your situation. Eye Surgery Today provides the foundational knowledge to help you enter that conversation prepared.





