Lens replacement is a surgical procedure that removes the eye’s natural crystalline lens and replaces it with an artificial intraocular lens (IOL) implant designed to restore clear vision. When cataracts, presbyopia, or other conditions compromise the natural lens beyond functional use, this procedure addresses the root cause of vision loss rather than compensating for it externally.
This guide covers the natural lens and why it may need replacing, surgical removal and implant placement techniques, IOL types and how they serve different visual goals, the recovery and healing timeline, potential benefits and risks, and candidacy considerations.
The natural lens is a biconvex, elastic structure that focuses light onto the retina through a process called accommodation. Cataracts remain one of the leading causes of treatable blindness worldwide, and when the lens can no longer provide functional vision, surgical intervention becomes necessary.
Surgeons remove the natural lens primarily through phacoemulsification, sometimes assisted by a femtosecond laser, both performed through small corneal incisions that promote faster healing. The new IOL is then folded, inserted through the same incision, and positioned within the preserved capsular bag.
IOL options include monofocal, multifocal, extended depth of focus, toric, and accommodating designs. Each type may offer distinct advantages for distance clarity, spectacle independence, or astigmatism correction depending on individual visual goals.
Most patients experience progressive visual improvement within the first few weeks, with full stabilization typically occurring between one and three months. Temporary glare or halos are common early on but rarely persist beyond the first year.
Risks such as posterior capsule opacification, infection, and implant dislocation vary in likelihood, and candidacy depends on corneal health, axial length, macular status, and any history of prior refractive surgery.
What Is the Natural Lens and Why Does It Need Replacing?
The natural lens is a transparent structure inside the eye that focuses light onto the retina to produce clear vision. When disease or aging compromises this lens, surgical replacement becomes necessary.
What Does Your Natural Lens Do Inside the Eye?
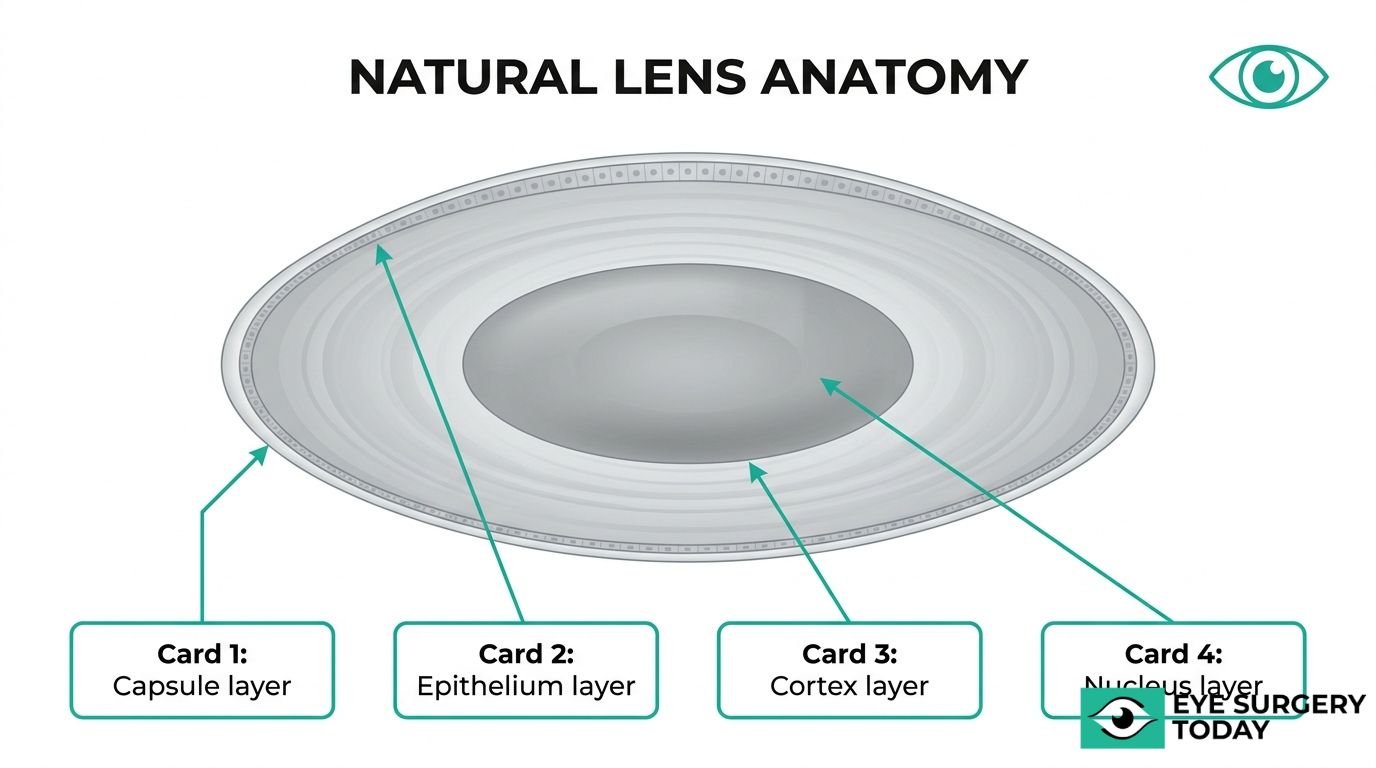
Your natural lens focuses incoming light onto the retina, enabling sharp vision at varying distances. According to BMJ Open Ophthalmology, the human crystalline lens is a transparent, biconvex, and elastic organ located in the posterior chamber, supported by the vitreous body and suspended by zonules attached between the pars plana and the equatorial lens capsule.
The crystalline lens contains four distinct structures:
- The lens capsule, a basement membrane containing type IV collagen
- The epithelium, which maintains metabolic activity
- The cortex, composed of younger lens fibers
- The nucleus, formed by older, compacted fibers at the center
This layered architecture allows the lens to change shape through accommodation. During this process, ciliary muscle contraction relaxes the zonules, permitting the lens to become more convex for near focus. Over time, however, the lens gradually loses this elasticity, which is why reading vision often declines with age.
What Conditions Can Cause the Natural Lens to Fail?
The conditions that can cause the natural lens to fail include cataracts, presbyopia, and less common disorders that compromise lens transparency or flexibility.
Cataracts remain the leading cause of treatable blindness worldwide. In 2020, among the 43.3 million blind individuals globally, 17.0 million cases (39.6%) were attributable to cataracts, according to the Institute for Health Metrics and Evaluation (IHME).
Other conditions that may impair natural lens function include:
- Presbyopia: age-related loss of accommodation that reduces near focusing ability
- Traumatic lens damage: blunt or penetrating eye injuries that disrupt lens integrity
- Metabolic cataracts: lens opacification associated with systemic conditions such as diabetes
- Congenital lens abnormalities: structural defects present from birth that affect clarity or position
When the natural lens can no longer provide functional vision, surgical replacement with an intraocular lens implant offers a well-established path to restored sight. Understanding how that removal and replacement process works is the next step.
How Does a Surgeon Remove the Natural Lens?
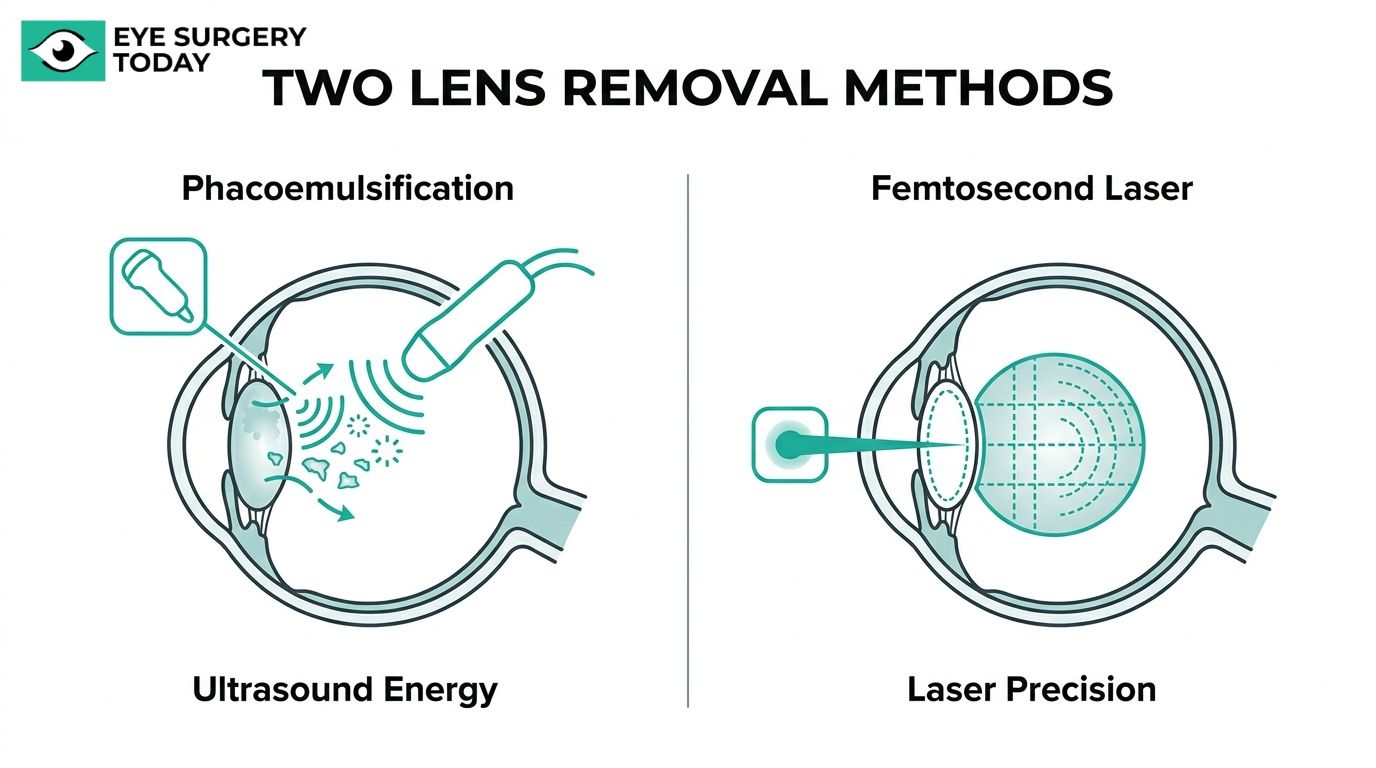
A surgeon removes the natural lens by breaking it into small fragments and suctioning them out through a tiny incision. The two primary techniques are phacoemulsification and femtosecond laser-assisted removal.
What Happens During Phacoemulsification?
Phacoemulsification uses ultrasonic energy to break the natural lens into tiny fragments for removal. The surgeon creates a small corneal incision, typically 2.2 to 2.8 millimeters wide, and inserts a thin probe into the eye. This probe emits high-frequency ultrasound waves that emulsify the clouded lens nucleus and cortex into microscopic pieces.
As the lens material liquefies, the same probe simultaneously aspirates the fragments through its hollow center. Because the capsular bag is preserved intact during this process, it serves as the support structure for the new intraocular lens implant placed afterward.
The entire removal phase generally takes only a few minutes once the surgeon gains access. Phacoemulsification remains the most widely performed cataract removal technique worldwide, largely because the small incision promotes faster healing and rarely requires sutures. For most patients, this approach offers a well-established balance of precision and safety that few surgical techniques can match.
What Happens During Femtosecond Laser-Assisted Removal?
Femtosecond laser-assisted removal uses an image-guided laser to perform key steps of lens extraction before ultrasonic energy is applied. The laser creates precise corneal incisions, a perfectly circular opening in the anterior capsule (capsulotomy), and softens or fragments the lens nucleus into a predefined pattern.
By pre-fragmenting the lens, the procedure may reduce the amount of ultrasonic energy needed during the subsequent phacoemulsification step. This can be particularly useful in dense cataracts, where conventional ultrasound alone requires more energy. According to a study published in Ophthalmology (Journal of the American Academy of Ophthalmology), femtosecond laser-assisted cataract surgery is not inferior to conventional phacoemulsification in terms of visual outcomes, patient-reported health, and safety at three months post-operation.
The laser’s precision in capsulotomy creation may also contribute to more predictable intraocular lens centration. In practice, the choice between laser-assisted and conventional phacoemulsification often depends on the complexity of the case and the surgeon’s clinical judgment.
With the natural lens removed, the next step involves placing the new intraocular lens implant.
What Is an Intraocular Lens Implant?
An intraocular lens implant is a small, artificial lens placed inside the eye to replace the natural crystalline lens after it has been removed during surgery. Made from biocompatible materials such as acrylic, silicone, or hydrophobic polymers, this permanent optical device restores the eye’s ability to focus light onto the retina. Unlike contact lenses or glasses, which sit outside the eye, an intraocular lens implant functions from within the posterior chamber, occupying the same position the natural lens once held.
Once folded and inserted through a micro-incision, the IOL unfolds inside the capsular bag and remains stable without any sensation to the patient. Each implant is calculated to a specific optical power based on the individual eye’s measurements, including corneal curvature and axial length. This precision is what allows the lens to correct refractive errors such as nearsightedness, farsightedness, or astigmatism at the time of surgery.
The technology behind these implants continues to advance. Johnson & Johnson’s TECNIS PureSee IOL, for example, became the first U.S. FDA-approved non-diffractive extended depth of focus lens that provides a continuous range of vision without a warning on loss of contrast sensitivity. Innovations like this extend the functional range of a single implant, helping patients achieve greater independence from glasses at near, intermediate, and distance vision.
For most recipients, an intraocular lens implant is a permanent, one-time placement that requires no maintenance or replacement. Understanding what this device is and how it functions provides the foundation for evaluating the different IOL types, surgical techniques, and visual outcomes covered throughout this guide.
What Are the Types of Intraocular Lens Implants?
The types of intraocular lens implants are monofocal, multifocal, extended depth of focus, toric, and accommodating IOLs. Each type addresses different visual needs and lifestyle goals.
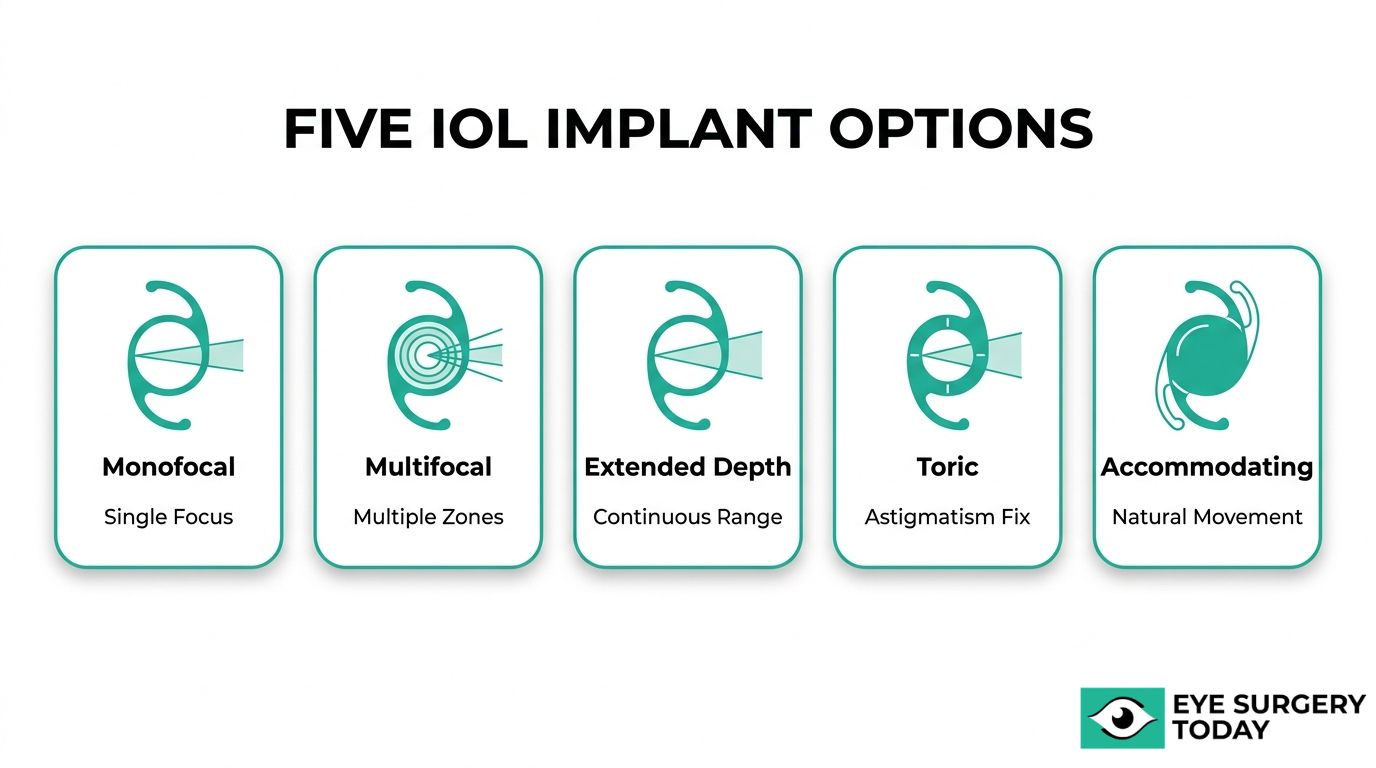
Monofocal IOL
A monofocal IOL is an intraocular lens designed to provide clear vision at one fixed focal point, typically set for distance. Most surgeons consider it the standard lens choice during cataract surgery because of its reliable optical quality and well-established track record. Patients who receive a monofocal IOL generally still need reading glasses or bifocals for intermediate and near tasks. Despite this limitation, the simplicity of a single-focus design tends to produce excellent contrast sensitivity and minimal visual disturbances like halos or glare. For patients who prioritize sharp distance vision and are comfortable wearing glasses for close work, monofocal lenses remain a highly practical option.
Multifocal IOL
A multifocal IOL is an intraocular lens that uses concentric rings or zones to split incoming light into multiple focal points, providing vision at near, intermediate, and far distances simultaneously. This design can significantly reduce dependence on glasses after surgery. However, because light is divided across focal zones, some patients may notice halos or glare around lights, particularly at night. According to a 2023 review in the Journal of Clinical Medicine, EDOF and multifocal IOLs may result in a loss of contrast sensitivity compared to monofocal controls. Careful patient selection is essential; individuals with realistic expectations about potential visual trade-offs tend to achieve the highest satisfaction with multifocal lenses.
Extended Depth of Focus IOL
An extended depth of focus IOL is an intraocular lens that elongates a single focal point rather than splitting light into multiple zones. This approach creates a continuous range of clear vision from distance through intermediate, with functional near vision in most lighting conditions. Unlike traditional multifocal designs, EDOF lenses may produce fewer halos and glare disturbances. The TECNIS PureSee IOL, announced by Johnson & Johnson, is the first and only U.S. FDA-approved non-diffractive EDOF lens that provides a continuous range of vision without a warning on loss of contrast sensitivity. For patients who want reduced spectacle dependence with minimal optical side effects, EDOF technology represents one of the most balanced options currently available.
Toric IOL
A toric IOL is an intraocular lens specifically designed to correct corneal astigmatism at the time of cataract or lens replacement surgery. Astigmatism occurs when the cornea has an irregular curvature, causing blurred or distorted vision at all distances. A toric lens has different optical powers along its meridians, which counteract the corneal irregularity when precisely aligned during implantation. Rotational stability is critical; even small degrees of misalignment can reduce the astigmatism correction. For patients with moderate to significant corneal astigmatism, a toric IOL can deliver noticeably sharper distance vision compared to a standard spherical lens, making it a worthwhile consideration during the preoperative planning discussion.
Accommodating IOL
An accommodating IOL is an intraocular lens designed to shift position inside the eye in response to ciliary muscle contraction, mimicking the natural focusing mechanism of the crystalline lens. By moving slightly forward when the eye attempts to focus on near objects, this lens type aims to provide a range of vision without relying on diffractive or refractive zones. In practice, the range of near focus tends to be more modest compared to multifocal or EDOF designs, and some patients may still require reading glasses for fine print. Accommodating lenses suit individuals who want a more natural visual experience with fewer optical disturbances, though setting realistic expectations about near vision capability remains important.
Understanding the distinct strengths of each IOL type helps guide the conversation with your surgeon about which lens best fits your vision goals.
How Does the Surgeon Place the New Lens Implant?
The surgeon places the new lens implant by folding it into an inserter device and guiding it through the same small incision used to remove the natural lens. The subsections below cover capsular bag positioning and procedure timing.
How Is the IOL Positioned Inside the Capsular Bag?
The IOL is positioned inside the capsular bag by inserting the folded lens through a micro-incision and allowing it to unfold within the thin, transparent membrane that originally held the natural lens. According to a step-by-step guide published by MillennialEYE, standard IOL implantation involves placing the lens haptics within the capsular bag, often using an inserter angled so the leading haptic enters under the far side of the capsular bag.
Once the leading haptic clears the capsular rim, the trailing haptic follows and tucks beneath the opposite edge. The two haptics, which are flexible arms extending from the optic, center the lens and hold it stable. Gentle pressure from the capsular bag keeps the IOL in its intended optical position behind the iris.
When capsular support is compromised, surgeons may use alternative fixation methods, such as intrascleral haptic fixation, to secure the lens directly to the sclera. Proper centration within the capsular bag remains the single most important factor for predictable refractive outcomes after implantation.
How Long Does the Implant Procedure Take?
The implant procedure typically takes between 15 and 30 minutes per eye for most patients. The actual IOL insertion step, from loading the lens into the cartridge to confirming centration inside the capsular bag, accounts for only a few minutes of that total time.
Several factors can influence overall duration:
- Lens type complexity: Toric IOLs require precise rotational alignment, which may add time for axis marking and verification.
- Capsular bag condition: A weakened or compromised capsule demands more careful manipulation during haptic placement.
- Surgical technique: Femtosecond laser-assisted approaches include a laser pretreatment phase before the manual implantation step.
Most patients spend additional time in the preoperative area for dilation and anesthesia preparation, and briefly in recovery for initial post-surgical monitoring. The brevity of the implantation itself is one reason lens replacement is performed as an outpatient procedure, with patients returning home the same day.
With the implant secured, the focus shifts to what happens during the immediate post-operative period.
What Should You Expect Right After Lens Replacement?
Right after lens replacement, you may experience mild visual disturbances and temporary discomfort as the eye begins healing. The sections below cover early sensory experiences and standard postoperative medications.
What May You See and Feel in the First Few Hours?
In the first few hours after lens replacement, you may see mild haziness, notice light sensitivity, and feel a gritty or watery sensation in the operated eye. These responses are normal as the cornea and surrounding tissues recover from the surgical process.
Bright lights may appear surrounded by halos or streaks, a phenomenon known as positive dysphotopsia. Colors often seem noticeably more vivid once the clouded natural lens has been removed, since the new intraocular lens transmits light more efficiently. Some patients also report a mild foreign-body sensation, which typically results from the small incision site rather than the implant itself.
Mild tearing and slight redness around the eye are common during this initial period. Vision usually fluctuates between clear and blurry as the pupil returns to its normal size after dilation. Most of these early symptoms begin improving within hours, though intermittent blurriness can persist into the next day. For most patients, keeping the protective eye shield in place and avoiding rubbing the eye are the two most important actions during this window.
What Medications and Eye Drops Are Typically Prescribed?
The medications and eye drops typically prescribed after lens replacement include antibiotic drops, anti-inflammatory drops, and sometimes a mild steroid regimen. Each serves a distinct role in protecting the healing eye.
- Antibiotic eye drops help prevent bacterial infection, including endophthalmitis, during the vulnerable early postoperative period.
- Corticosteroid eye drops reduce inflammation inside the eye, which can otherwise delay healing or cause complications such as cystoid macular edema.
- Nonsteroidal anti-inflammatory (NSAID) eye drops may be prescribed alongside steroids to further control swelling and manage discomfort.
- Lubricating drops help relieve dryness and the gritty sensation that commonly follows surgery.
According to research published in the Journal of Clinical Medicine, the incidence of endophthalmitis has shown a decreasing trend over time, particularly with intracameral antibiotic administration. Strict adherence to the prescribed drop schedule is one of the simplest yet most impactful things patients can do to support a smooth recovery.
Understanding the immediate postoperative period helps set realistic expectations as the eye enters its longer healing phase.
How Does the Eye Heal Around the New Implant?
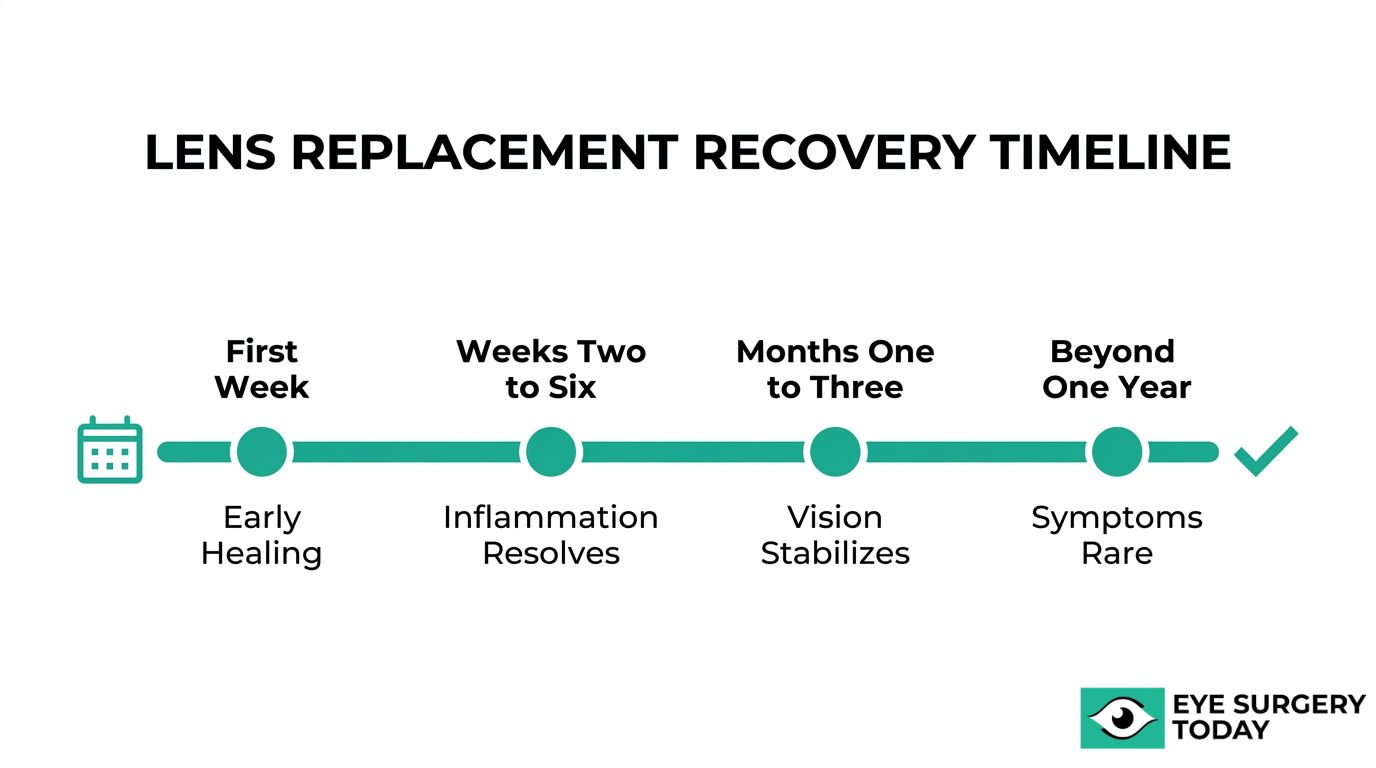
The eye heals around the new implant through a gradual process that unfolds over several weeks. Recovery milestones include early tissue stabilization, inflammation resolution, and final visual refinement. Understanding specific recovery processes is crucial for any ophthalmic procedure, including specialized treatments like eyelid surgery which has its own distinct healing timeline.
What Happens During the First Week of Recovery?
The first week of recovery involves the eye’s initial inflammatory response settling while the capsular bag begins securing the intraocular lens implant in position. Mild redness, light sensitivity, and blurred vision are common during this stage, as the corneal incision starts closing and internal swelling subsides.
Patients typically use prescribed anti-inflammatory and antibiotic eye drops to manage this healing phase. Avoiding heavy lifting, rubbing the eye, and exposure to dust or water helps protect the surgical site. Most people notice incremental visual improvement within the first few days, though fluctuations are normal as the eye adjusts. Following the postoperative drop schedule closely during this window sets the foundation for a smoother recovery overall.
What Happens During Weeks Two Through Six?
Weeks two through six represent the period when residual inflammation resolves and the capsular bag fully contracts around the IOL haptics, anchoring the implant in its permanent position. Swelling in the cornea and surrounding tissues continues to diminish, which progressively sharpens visual clarity.
During this phase, your ophthalmologist may begin tapering anti-inflammatory eye drops based on healing progress. Activities like moderate exercise and screen use can often resume, though protective eyewear remains advisable in dusty or bright environments. Any lingering scratchiness or dryness typically improves as the surface epithelium finishes remodeling. From a clinical standpoint, this middle recovery window is where the most meaningful visual gains occur for the majority of patients.
When Does Vision Typically Stabilize After Surgery?
Vision typically stabilizes after surgery within one to three months, though minor refinements can continue for up to six months in some cases. Early visual disturbances, particularly glare and halos, are common but usually temporary. According to a study published in the Journal of Clinical Medicine, up to 67% of patients may experience positive dysphotopsia immediately after cataract surgery, yet persistent symptoms lasting beyond one year occur in only roughly 2.2% of cases.
Your ophthalmologist may schedule a final refraction assessment once the eye has fully healed, determining whether any residual prescription correction is needed. Patients frequently ask whether lens replacement is permanent; the IOL itself is designed to last a lifetime, though conditions like posterior capsule opacification can develop later and require a brief laser procedure. For most patients, the period between weeks six and twelve marks the point where everyday vision feels consistently clear and reliable.
With healing complete, the long-term benefits of the new implant become apparent.
What Are the Potential Benefits of a Lens Implant?
The potential benefits of a lens implant include improved distance vision, reduced dependence on glasses, and enhanced contrast and color perception.
How May a Lens Implant Help with Distance Vision?
A lens implant may help with distance vision by replacing a clouded or optically imperfect natural lens with a precisely powered intraocular lens (IOL) that restores clear focus at far distances. The type of IOL selected determines how much distance clarity improves.
Monofocal IOLs deliver sharp distance vision at a single focal point, while advanced designs extend that range further. The Alcon Vivity, a non-diffractive extended depth of focus (EDOF) IOL, utilizes X-WAVE technology to stretch and shift light, delivering monofocal-quality distance vision while also improving intermediate and near visual acuity. For patients with corneal astigmatism, toric IOLs can be particularly effective. According to ESCRS guidelines, toric IOLs should be considered in eyes with corneal astigmatism of 1.0D or more, as they provide significantly better distance visual acuity than non-toric lenses in these patients.
Even in complex cases, outcomes can be favorable. Refractive lens exchange in amblyopic eyes has been shown to safely improve corrected distance visual acuity in both hyperopic (farsighted) and myopic (nearsighted) patients, provided no other ocular pathology is present. For most patients, selecting the right IOL power and design is the single most important factor in achieving the distance vision they want.
How May a Lens Implant Help Reduce Dependence on Glasses?
A lens implant may help reduce dependence on glasses by correcting refractive errors that previously required external lenses. Multifocal and extended depth of focus IOLs split or stretch incoming light to cover multiple focal distances, allowing patients to see clearly at far, intermediate, and near ranges without reaching for spectacles.
According to a study published in the American Journal of Ophthalmology, refractive lens exchange has been shown to improve uncorrected visual acuity at far, intermediate, and near distances, leading to high levels of patient satisfaction. Toric IOL designs add astigmatism correction, which further reduces the need for glasses in patients who previously relied on cylinder-corrected prescriptions.
Complete spectacle independence is not guaranteed for every patient; some may still prefer reading glasses in low-light conditions or for prolonged near tasks. Still, modern premium IOLs offer the most reliable path to meaningful glasses use reduction after lens replacement.
How May a Lens Implant Help with Contrast and Color?
A lens implant may help with contrast and color by removing the yellowed, opacified natural lens that filters and dulls incoming light. A cataract progressively absorbs shorter wavelengths, which mutes blues and greens and reduces overall contrast sensitivity. Once that barrier is replaced with a clear synthetic IOL, the full visible spectrum reaches the retina again.
Many patients describe colors as noticeably more vivid and whites as brighter within the first days after surgery. Contrast sensitivity, the ability to distinguish objects from similarly shaded backgrounds, can also improve because the new lens transmits light without the scatter that a cataract creates. Not all IOL designs affect contrast equally, however. Some diffractive multifocal lenses may slightly reduce contrast sensitivity compared to monofocal designs, so the choice of implant matters.
For patients whose daily activities depend on accurate color perception or sharp contrast, such as driving at night, this benefit is often among the most immediately noticeable improvements after lens replacement. Understanding these visual gains sets the stage for weighing possible risks.
What Are the Possible Risks and Complications?
Some of the possible risks and complications of lens replacement include posterior capsule opacification, infection, implant dislocation, and cystoid macular edema. Each complication varies in likelihood and severity.
What Is Posterior Capsule Opacification?
Posterior capsule opacification (PCO) is a gradual clouding of the thin membrane left behind the intraocular lens after cataract surgery. Residual lens epithelial cells can proliferate across the posterior capsule, scattering light and causing blurred vision that mimics the original cataract symptoms.
According to Ophthalmology Times, PCO is the most common late complication of cataract surgery, with incidence rates ranging from less than 5% to as high as 50% depending on IOL material and design. Hydrophobic acrylic lenses and sharp-edged optic designs have been associated with lower PCO rates compared to older lens styles.
When PCO does develop, a quick in-office YAG laser capsulotomy can restore clear vision within minutes. For most patients, this remains a straightforward correction rather than a serious setback.
What Are the Signs of Infection or Endophthalmitis?
The signs of infection or endophthalmitis include increasing eye pain, worsening redness, significant vision loss, lid swelling, and discharge that develops within days to weeks after surgery. Endophthalmitis is a severe intraocular infection that, without prompt treatment, can cause permanent vision damage.
Although rare, certain precautions have reduced its occurrence. Intracameral antibiotic administration during surgery has been associated with a decreasing trend in endophthalmitis incidence following phacoemulsification, according to a review published in the Journal of Clinical Medicine.
Any patient who experiences a sudden drop in vision accompanied by pain after lens replacement should contact their surgeon immediately. Early intervention with intravitreal antibiotics may help preserve visual function.
Can the Implant Shift or Dislocate After Surgery?
Yes, the implant can shift or dislocate after surgery, though this complication is uncommon. Late IOL dislocation may occur months or years after the procedure, often related to weakening of the zonular fibers that support the capsular bag.
Risk factors include:
- Pseudoexfoliation syndrome
- Prior ocular trauma
- High myopia
- Previous vitreoretinal surgery
When the capsular bag can no longer provide adequate support, intrascleral IOL fixation techniques may be used to secure the haptics directly to the sclera, restoring lens stability. Minor shifts that do not affect vision are typically monitored rather than surgically corrected.
In clinical practice, careful preoperative assessment of zonular integrity is one of the most effective ways to reduce dislocation risk.
What Is Cystoid Macular Edema After Lens Replacement?
Cystoid macular edema (CME) after lens replacement is a condition in which fluid accumulates in cyst-like spaces within the macula, the central part of the retina responsible for sharp vision. This swelling can cause blurred or distorted central vision in the weeks following surgery.
CME may develop when surgical inflammation triggers breakdown of the blood-retinal barrier, allowing fluid to leak into macular tissue. Patients with diabetes, uveitis, or a history of retinal vein occlusion may face a higher risk.
Treatment typically involves topical anti-inflammatory eye drops, such as NSAIDs and corticosteroids, prescribed in the postoperative period. Most cases of CME resolve with medical management, though persistent edema may require additional interventions.
With an understanding of these potential complications, knowing who qualifies for the procedure helps set realistic expectations from the start.
Who Is a Good Candidate for Lens Replacement Surgery?
A good candidate for lens replacement surgery typically has healthy corneas, appropriate axial length, and no significant macular disease. Eligibility also depends on prior surgical history and specific eye health conditions.
What Eye Health Conditions May Affect Eligibility?
Eye health conditions that may affect eligibility for lens replacement surgery include macular disease, corneal irregularities, and uncontrolled glaucoma. Significant retinal pathology can limit the visual benefit of a new intraocular lens, while corneal conditions may compromise surgical precision and postoperative outcomes.
Factors your ophthalmologist may evaluate include:
- Corneal health: Conditions such as keratoconus, Fuchs’ dystrophy, or prior corneal scarring can alter how light passes through the eye and may complicate IOL power calculations.
- Macular disease: Active macular degeneration or diabetic macular edema may reduce the visual gains a lens implant can provide.
- Axial length: Eyes that are unusually short or long require more precise IOL calculations to achieve the target refraction.
- Glaucoma severity: Advanced glaucoma with significant optic nerve damage may limit functional improvement after surgery.
According to the American Academy of Ophthalmology, candidate eligibility for refractive lens exchange depends on corneal health, axial length, and the absence of significant macular disease. In clinical practice, a thorough preoperative workup that screens for these conditions is one of the most important steps in achieving a successful outcome.
What If You Have Had Previous Refractive Surgery?
Previous refractive surgery, such as LASIK or PRK, does not automatically disqualify you from lens replacement. However, prior corneal procedures alter the eye’s surface curvature, which makes calculating the correct IOL power significantly more complex.
The central challenge is that standard IOL formulas rely on corneal measurements that no longer reflect the eye’s true refractive state after laser correction. Even small calculation errors can lead to a refractive surprise, leaving a patient more nearsighted or farsighted than expected after surgery.
Specialized tools help address this challenge. According to the American Academy of Ophthalmology, the ASCRS post-refractive IOL calculator is a recommended tool for improving calculation accuracy in patients with prior corneal refractive surgery. Surgeons may also request pre-LASIK records, when available, to refine their measurements further.
For patients who have previously had refractive surgery, the importance of precise IOL selection cannot be overstated; accurate power calculation remains the primary determinant of satisfaction after the procedure. With the right preoperative planning, many post-LASIK and post-PRK patients can still achieve excellent visual outcomes from lens replacement.

How Does Lens Replacement Compare to Wearing Glasses?
Lens replacement compares to wearing glasses by offering a permanent optical correction built into the eye, while glasses provide an external, adjustable solution that requires ongoing updates.
Glasses correct vision by bending light before it enters the eye. Each prescription addresses a specific refractive error at a fixed point in time, so lenses need replacing as vision changes. Lens implants, by contrast, replace the eye’s internal optics entirely. A monofocal, multifocal, toric, or extended depth of focus IOL is selected to match the patient’s visual needs, and once placed inside the capsular bag, it becomes a permanent part of the eye’s optical system.
According to a study published in the Journal of Refractive Surgery, quality of life scores are typically lowest in spectacle wearers compared to those who have undergone refractive surgery or wear contact lenses, particularly for those with higher refractive corrections. This gap tends to widen as prescriptions grow stronger, since thicker lenses introduce more peripheral distortion and weight.
From a practical standpoint, glasses remain the safest, most reversible option for mild refractive errors. However, for patients whose cataracts or presbyopia have progressed beyond comfortable spectacle correction, a lens implant can address the root cause rather than compensating for it externally. The trade-off is that surgery carries risks, including posterior capsule opacification and temporary dysphotopsia, that glasses never introduce.
For many patients over 50 with moderate to high refractive error or early cataract changes, lens replacement may offer a more lasting improvement in functional vision than progressively stronger spectacle prescriptions. The best choice depends on individual eye health, lifestyle demands, and tolerance for surgical risk, which is why a thorough evaluation with an ophthalmologist remains essential before deciding.
How Can Expert-Reviewed Guidance Help You Prepare?
Expert-reviewed guidance can help you prepare by turning complex surgical details into clear, actionable knowledge. The sections below cover how Eye Surgery Today supports your decision-making and the essential takeaways about lens replacement.
Can Eye Surgery Today Help You Understand Your Options?
Yes, Eye Surgery Today can help you understand your options. The platform was built by nationally recognized ophthalmology key opinion leaders specifically to bridge the gap between clinical expertise and patient understanding. Every guide, article, and resource on the site translates complex lens replacement concepts into accessible language, covering IOL types, surgical techniques, recovery timelines, and candidacy factors.
Rather than relying on fragmented information from general health sites, readers gain surgeon-level insights. Eye Surgery Today offers educational articles, surgeon profiles, and resources like “Cataract Surgery Step by Step: What Happens During the Procedure” to help patients approach consultations with confidence. Having a trusted, evidence-based foundation before meeting your ophthalmologist can make the difference between feeling overwhelmed and feeling prepared.
What Are the Key Takeaways About Lens Replacement?
The key takeaways about lens replacement center on understanding the procedure, selecting the right implant, and setting realistic recovery expectations. According to OCL Vision’s frequently asked questions resource, patient concerns often focus on the safety profile of premium IOLs, the difference between refractive lens exchange and cataract surgery, and the likelihood of needing glasses after the procedure.
The most important points to carry forward include:
- Lens replacement removes a clouded or dysfunctional natural lens and replaces it with an intraocular lens implant tailored to your vision needs.
- IOL options range from monofocal and toric to multifocal and extended depth of focus designs, each suited to different visual goals.
- Recovery typically progresses through defined stages, with most visual improvement occurring within the first few weeks.
- Candidacy depends on corneal health, the absence of significant macular disease, and accurate preoperative measurements.
- Temporary visual phenomena like glare or halos are common early on but rarely persist long term.
For anyone considering this procedure, preparation starts with reliable information. Eye Surgery Today provides the surgeon-led educational foundation to help you navigate every stage of the lens replacement journey with clarity.
