A cataract consultation is a specialized appointment where your ophthalmologist evaluates lens opacity, discusses surgical timing, and helps you select an intraocular lens matched to your visual goals.
This guide covers recognizing when you need a consultation, understanding your diagnosis and surgical candidacy, comparing IOL options, evaluating the procedure and its risks, planning for recovery, navigating costs and insurance, and assessing your surgeon’s qualifications.
Knowing when symptoms like blurred vision, glare, or faded colors begin limiting daily tasks such as driving or reading can help you determine whether a dedicated cataract evaluation is more appropriate than a routine eye exam. Early assessment may give your surgeon more flexibility in planning.
Your diagnosis involves more than confirming a cataract exists. The specific cataract type, its current stage on standardized grading scales, and whether coexisting conditions like macular degeneration or glaucoma contribute to vision loss all shape the surgical approach and expected outcomes.
Candidacy depends on your full health profile. Diabetes, prior LASIK, dry eye, and other systemic or ocular conditions can influence technique selection, lens choice, and healing timelines. Surgical sequencing for bilateral cataracts also requires individualized planning.
IOL selection is one of the most consequential decisions in the process. Options range from standard monofocal lenses to multifocal, extended depth of focus, toric, and light adjustable designs; each carries distinct trade-offs in spectacle independence, visual disturbances, and out-of-pocket cost.
Understanding procedural details, including technique differences between phacoemulsification and femtosecond laser-assisted surgery, anesthesia options, and complication management protocols, helps you evaluate both the surgery and the surgeon performing it.
Recovery planning, insurance coverage, premium lens financing, and verifying your surgeon’s credentials and volume round out the preparation that may turn a potentially overwhelming consultation into a focused, productive conversation.
How Do You Know You Are Ready for a Cataract Consultation?
You are ready for a cataract consultation when vision changes begin interfering with everyday tasks. The sections below cover which symptoms warrant evaluation and when a consultation offers more value than a routine eye exam.
What Symptoms Suggest Your Cataracts Need Evaluation?
The symptoms that suggest your cataracts need evaluation are those that interfere with daily activities you rely on, such as driving at night, reading, or working at a computer. Blurred vision that no longer improves with an updated glasses prescription is often the earliest functional warning sign. Increased sensitivity to glare, halos around headlights, faded color perception, and frequent prescription changes within a short period can all point to progressing lens opacity.
According to the American Academy of Ophthalmology Preferred Practice Patterns, surgical appropriateness is based on indicators of visual acuity and functional impairment, such as difficulty with glare, halos, or decreased contrast sensitivity. If you notice any combination of these changes affecting how you perform routine tasks, that pattern of functional decline signals it may be time to move beyond monitoring and seek a dedicated cataract evaluation. Waiting until vision loss becomes severe is unnecessary; earlier assessment gives your surgeon more options.
When Should You Schedule a Consultation Versus a Routine Eye Exam?
You should schedule a cataract consultation instead of a routine eye exam when your symptoms actively limit daily function, not when you simply need a prescription update. A routine exam screens for eye health and refractive error. A cataract consultation, by contrast, focuses specifically on lens clarity, surgical timing, and intraocular lens selection.
The distinction matters because Medicare covers cataract surgery when the cataract causes symptomatic impairment of visual function that limits a patient’s ability to perform activities of daily living, such as reading, driving, or vocational tasks, according to AARP’s 2026 Medicare coverage guide. If your optometrist has already identified a cataract and your vision difficulties persist despite new glasses, requesting a surgical consultation is the appropriate next step. In clinical practice, patients who schedule consultations proactively tend to have more time to weigh lens options and plan recovery around their schedules.
With a clear sense of when to seek evaluation, the next step is understanding what to ask about your specific cataract diagnosis.
What Should You Ask About Your Cataract Diagnosis?
You should ask about the specific type of cataract, its current stage of progression, and whether the cataract is the sole cause of your vision changes. These three questions shape every decision that follows.
What Type of Cataract Do You Have?
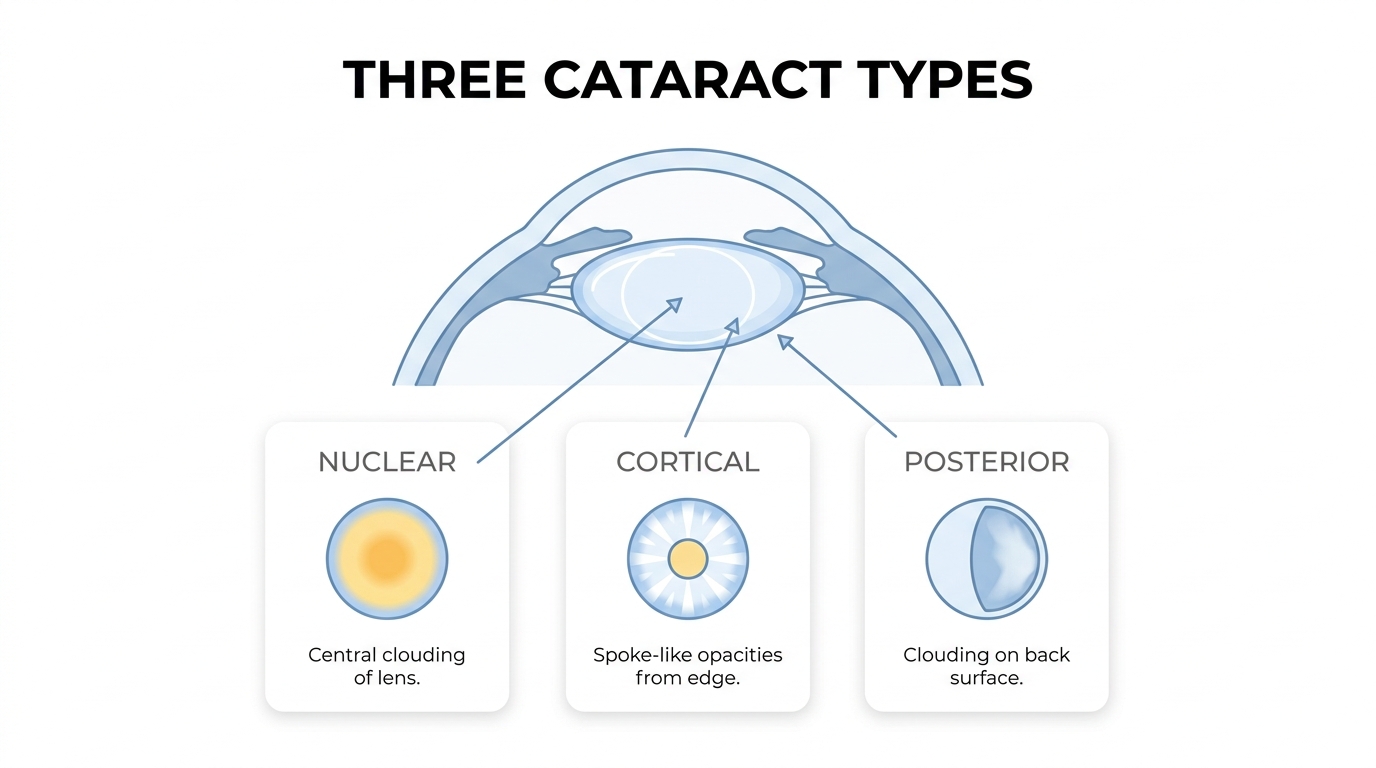
The type of cataract you have determines how quickly your vision may decline and which symptoms you experience first. There are three main types:
- Nuclear sclerotic cataracts develop in the central lens, causing gradual yellowing and blurred distance vision.
- Cortical cataracts form as spoke-like opacities in the lens periphery, often producing glare as the earliest complaint.
- Posterior subcapsular cataracts (PSC) appear on the back surface of the lens and can reduce visual acuity earlier and more rapidly than other types, according to StatPearls (NCBI).
Knowing your cataract type helps you understand the timeline. PSC, for example, may warrant earlier surgical discussion, while nuclear cataracts often progress slowly over years. Ask your surgeon to identify the specific type during your exam so you can set realistic expectations for how your vision may change.
How Advanced Is Your Cataract Right Now?
How advanced your cataract is right now directly affects whether monitoring or surgery is the appropriate next step. Ophthalmologists grade cataract severity using standardized scales, with the Lens Opacities Classification System III (LOCS III) being the most widely accepted. This system scores nuclear opalescence, nuclear color, cortical involvement, and posterior subcapsular changes on a decimal scale.
Ask your surgeon where your cataract falls on this grading spectrum. An early-stage cataract with minimal functional impact may only need periodic monitoring, while a moderate or advanced cataract causing measurable vision loss could indicate surgical timing is approaching. The grading also establishes a baseline, making it easier to track progression at future visits.
Is Your Vision Loss Caused Entirely by the Cataract?
Vision loss is not always caused entirely by the cataract. Conditions such as macular degeneration, glaucoma, and diabetic retinopathy can contribute to reduced vision independently or alongside a cataract. A comprehensive diagnostic workup is essential because removing a cataract will not restore vision lost to a separate underlying condition.
Your ophthalmologist can identify a cataract as any opacification of the crystalline lens observable through a dilated pupil using a slit lamp biomicroscope, as defined by the Centers for Medicare and Medicaid Services (CMS). However, additional testing, including optical coherence tomography and visual field analysis, may be needed to rule out coexisting pathology. This distinction matters: if another condition is the primary driver of your symptoms, surgical expectations must be adjusted accordingly.
Understanding the full diagnostic picture before proceeding to surgery ensures you and your surgeon share realistic outcome goals.
What Questions Should You Ask About Your Candidacy for Surgery?
The questions you should ask about your candidacy for surgery focus on how your eye health, systemic conditions, and surgical history may affect outcomes. The following subsections cover existing eye conditions, diabetes and other health factors, previous refractive surgery, and bilateral treatment sequencing.
Do Any Existing Eye Conditions Affect Your Surgical Options?
Existing eye conditions can significantly affect your surgical options for cataract removal. Conditions such as glaucoma, macular degeneration, and diabetic retinopathy may limit which intraocular lens types are appropriate or alter the expected visual outcome. For example, patients with macular disease may not benefit as much from premium multifocal IOLs because these lenses rely on healthy retinal function to deliver their full range of vision.
Dry eye syndrome, corneal dystrophies, and uveitis can also influence surgical timing and technique. Your ophthalmologist may recommend treating these conditions before scheduling cataract extraction to reduce complication risk. Asking specifically whether any coexisting eye diagnosis changes the expected benefit of surgery is one of the most practical questions a patient can raise during a consultation.
How Might Diabetes or Other Health Conditions Influence Your Outcome?
Diabetes and other systemic health conditions may influence your cataract surgery outcome in several ways. Diabetic retinopathy, in particular, can complicate both the procedure and the healing process. Elevated blood sugar levels are associated with increased inflammation, slower wound recovery, and a higher risk of postoperative macular edema.
Beyond diabetes, conditions such as autoimmune disorders and blood-thinning medication use can affect surgical planning. Your surgeon may coordinate with your primary care physician to optimize blood sugar control or adjust medications before the procedure. Patients should ask whether their systemic health status requires any preoperative clearance, additional testing, or modified postoperative monitoring. This conversation helps set realistic expectations for visual recovery.
Does Previous LASIK or Refractive Surgery Change the Approach?
Previous LASIK or refractive surgery does change the approach to cataract surgery. The primary challenge involves accurate IOL power calculation, because prior corneal reshaping alters the measurements surgeons rely on to select the correct lens. Without specialized formulas, there is a higher risk of refractive surprise, where the postoperative prescription differs from the intended target.
According to the American Society of Cataract and Refractive Surgery (ASCRS), post-refractive IOL calculators have been developed specifically to improve accuracy for these patients. Bringing records from your original LASIK procedure, including pre-LASIK corneal measurements, gives your surgeon critical data for more precise lens selection. Patients with prior radial keratotomy, PRK, or SMILE should raise this history early in the consultation so the surgical plan accounts for their altered corneal geometry.
Should Both Eyes Be Treated and in What Order?
Both eyes are typically treated in separate procedures rather than simultaneously. Most surgeons schedule the second eye surgery one to four weeks after the first, allowing time to assess the initial eye’s healing, refractive result, and any complications before proceeding.
This sequential approach offers a practical advantage: the outcome of the first eye can inform IOL selection for the second. If the refractive target lands slightly off in the first eye, your surgeon can adjust the lens power for the second to achieve better overall binocular vision. Patients should ask whether their specific situation warrants a shorter or longer interval between surgeries, particularly if one eye has a significantly more advanced cataract or if both eyes have different visual demands.
Understanding your candidacy profile lays the groundwork for the next critical decision: choosing the right intraocular lens.
What Should You Ask About Intraocular Lens Options?
You should ask about intraocular lens options that match your lifestyle, visual goals, and budget. The sections below cover monofocal versus premium IOLs, multifocal and EDOF designs, toric lenses for astigmatism, the Light Adjustable Lens, and how to choose between near and distance correction.
How Does a Standard Monofocal IOL Differ From a Premium IOL?
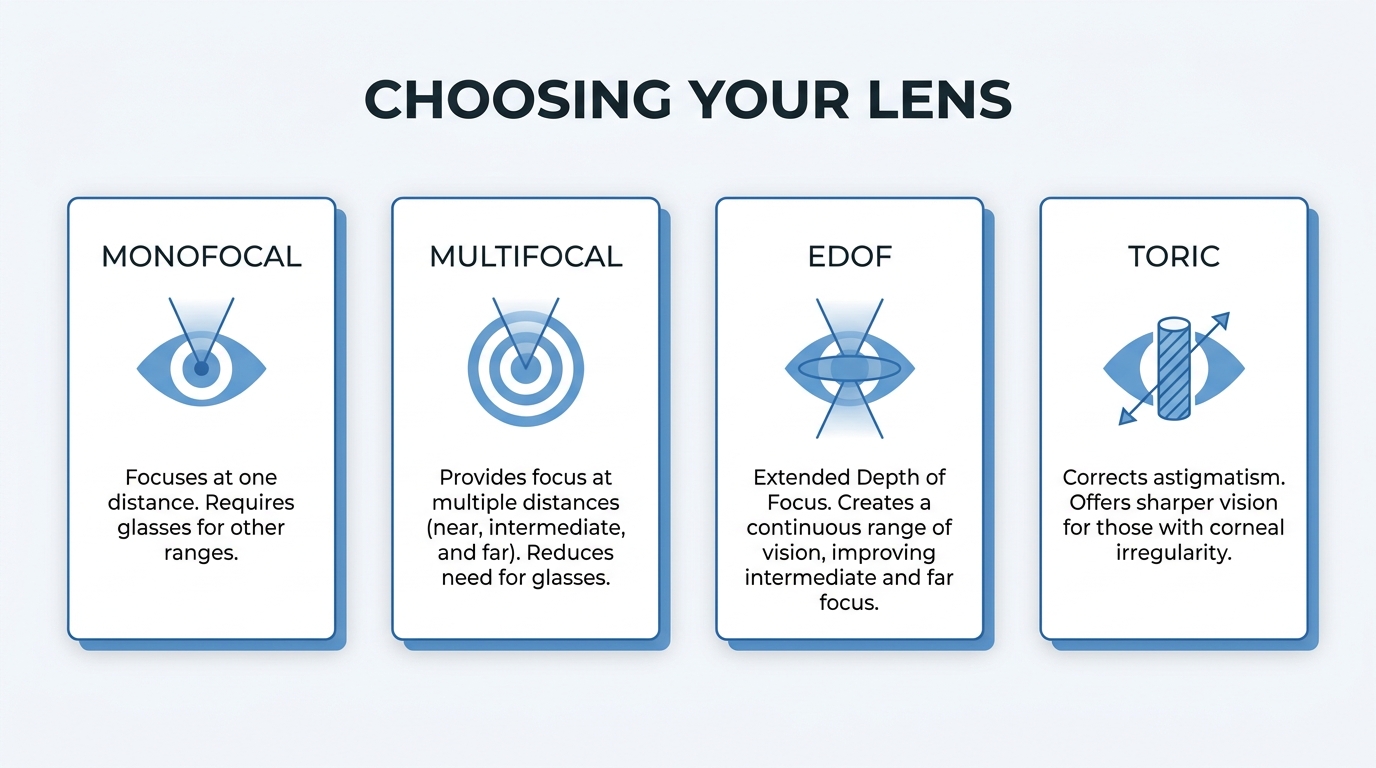
A standard monofocal IOL differs from a premium IOL in the number of focal points it provides. Monofocal lenses correct vision at one distance, typically far, so most patients still need reading glasses afterward. Premium IOLs, which include multifocal, extended depth of focus, and toric designs, aim to reduce dependence on glasses across multiple distances.
Cost structure also separates the two categories. According to Platte Medicare, Medicare’s policy for premium IOLs requires the patient to pay the out-of-pocket difference between a standard monofocal lens and the advanced technology lens, as these upgrades are considered elective enhancements. For patients weighing this decision, understanding which daily tasks matter most to you will help your surgeon recommend the right lens category.
Could a Multifocal or Extended Depth of Focus IOL Reduce Your Need for Glasses?
A multifocal or extended depth of focus IOL can reduce your need for glasses across multiple distances. Multifocal IOLs split incoming light into distinct focal zones for near, intermediate, and far vision, while EDOF lenses elongate a single focal point to create a continuous range.
According to the American Academy of Ophthalmology’s 2025 meeting findings, EDOF lenses provide a balanced visual outcome by improving intermediate vision while maintaining a lower incidence of visual disturbances compared to traditional trifocal multifocal lenses. Neither design guarantees complete spectacle independence, however, and some patients may still prefer lightweight readers for prolonged fine-print tasks. Asking your surgeon about your specific visual demands, particularly screen use and nighttime driving, helps determine which design may suit you best.
Is a Toric IOL Appropriate if You Have Astigmatism?
A toric IOL is appropriate if you have astigmatism that your surgeon considers clinically significant. Toric lenses contain built-in cylindrical correction that neutralizes corneal astigmatism at the time of cataract removal. Without this correction, residual astigmatism can leave vision blurry even after a successful surgery.
Precise alignment during implantation is critical, because even slight rotation of the toric lens reduces its corrective effect. Your surgeon will measure corneal curvature with advanced topography or biometry devices before recommending a toric option. Patients with irregular astigmatism from conditions like keratoconus may not be ideal candidates, so asking whether your astigmatism pattern is regular enough for a toric IOL is an important part of the consultation.
What Is a Light Adjustable Lens and Are You a Candidate?
The Light Adjustable Lens is a uniquely customizable IOL that allows your surgeon to fine-tune your prescription after cataract surgery rather than before. Unlike conventional lenses, the LAL uses photosensitive silicone material that changes shape when exposed to specific UV light treatments in the office, locking in your optimal refractive correction once healing stabilizes.
Candidacy typically requires a healthy macula, stable corneal measurements, and a commitment to wearing UV-protective glasses between adjustment sessions. Patients who have had unpredictable outcomes with prior refractive procedures or those who prioritize precise postoperative control over their prescription may benefit most. Because the adjustment process adds extra office visits, discussing whether the added precision justifies the time and cost is a practical question for your consultation.
How Do You Decide Between Near Vision and Distance Vision Correction?
You decide between near vision and distance vision correction by evaluating your daily visual priorities, existing refractive status, and tolerance for glasses. Patients who drive frequently or enjoy outdoor activities often prioritize distance correction, while those who read or do detailed handwork may prefer near-focused results.
Your eye’s natural lens changes can also influence this decision. As noted by the American Academy of Ophthalmology’s EyeWiki, nuclear sclerosis is the yellowing and hardening of the central lens that occurs slowly over years, sometimes temporarily improving near vision through a “second-sight” phenomenon. This effect disappears once the cataract is removed, so your post-surgical reading ability depends entirely on the IOL selected. Monovision, where one eye targets distance and the other near, is another strategy worth discussing if you tolerate the difference well during a trial.
Understanding your full range of IOL options prepares you to ask informed questions about the surgical procedure itself.
What Questions Should You Ask About the Surgical Procedure?
The questions you should ask about the surgical procedure cover technique selection, laser versus traditional methods, duration, and anesthesia type.
What Technique Will the Surgeon Use and Why?
The technique your surgeon will use depends on your cataract’s density, your eye anatomy, and the intraocular lens selected. Most surgeons perform phacoemulsification, which uses ultrasonic energy to break up and remove the clouded lens through a small incision. Some cases may call for femtosecond laser-assisted surgery, particularly when precise capsulotomy shape or lens fragmentation matters.
Ask your surgeon to explain why one approach suits your situation better than the other. Factors such as pupil dilation quality, corneal health, and the grade of lens opacity all influence technique selection. A surgeon who explains the reasoning behind their choice, rather than defaulting to a single method for every patient, demonstrates the kind of individualized care that typically leads to better outcomes.
How Does Femtosecond Laser-Assisted Surgery Compare to Traditional Phacoemulsification?
Femtosecond laser-assisted cataract surgery (FLACS) compares to traditional phacoemulsification by offering greater precision during key surgical steps, though both methods can produce excellent results. FLACS automates the corneal incision, capsulotomy, and initial lens fragmentation using a programmed laser, while conventional phacoemulsification relies entirely on the surgeon’s manual skill and ultrasonic energy.
According to a study published in Scientific Reports (Nature), FLACS achieves superior surgical precision in terms of effective phacoemulsification time and cumulative dissipated energy compared to conventional phacoemulsification. This reduced energy delivery may benefit patients with dense cataracts, where excessive ultrasonic power could stress the corneal endothelium.
However, FLACS typically costs more and adds time for laser docking. For most straightforward cataracts, skilled surgeons achieve comparable outcomes with either technique. The practical question to ask is whether the added precision of laser assistance provides a meaningful clinical advantage for your specific cataract grade.
How Long Does the Procedure Take?
The procedure takes approximately 10 to 20 minutes per eye in most cases. Cataract surgery is one of the fastest and most commonly performed operations in medicine, though the total time at the surgical facility is longer due to preparation, anesthesia administration, and post-procedure monitoring.
Patients often spend two to three hours at the facility overall. Unusually dense cataracts, small pupils, or the use of femtosecond laser assistance may extend the surgical portion slightly. Ask your surgeon whether any features of your case could affect timing, since knowing the expected duration helps reduce anxiety on the day of surgery.
What Type of Anesthesia Is Used During Cataract Surgery?
The type of anesthesia used during cataract surgery is typically topical or local. Most surgeons apply numbing eye drops (topical anesthesia) that eliminate pain while allowing the patient to remain awake and responsive. In some cases, a local anesthetic injection around the eye (peribulbar or retrobulbar block) provides deeper numbing for more complex procedures.
Light intravenous sedation often accompanies topical anesthesia to help patients relax without requiring general anesthesia. A 2025 study presented by the American Academy of Ophthalmology suggests that office-based cataract surgery using oral sedation may be a safe and effective alternative to traditional ambulatory surgery center settings for appropriate candidates. This trend could expand access while reducing facility-related costs.
Because fear of surgery remains a commonly cited barrier to seeking care, asking specifically about the sedation plan can ease concerns significantly. Understanding that the procedure involves minimal discomfort helps patients move forward with greater confidence.
What Should You Ask About Potential Risks and Complications?
You should ask about the most common complications, how posterior capsule opacification is managed, what happens if your refractive outcome misses the target, and how your surgeon handles rare but serious events.
What Are the Most Common Complications After Cataract Surgery?
The most common complications after cataract surgery include posterior capsule opacification, mild inflammation, elevated intraocular pressure, and residual refractive error. While cataract surgery carries one of the highest success rates of any surgical procedure, no operation is entirely without risk.
Posterior capsule opacification (PCO) is the most frequently reported post-operative issue. According to a 2025 bibliometric analysis published in Medicine (LWW), PCO incidence ranges from 5% to 50% within the first year after surgery, though it is correctable with a simple YAG laser capsulotomy. Less common intraoperative events, such as capsular tears and vitreous loss, occur in a small fraction of cases. Patients should discuss all possible complications with their surgeon to fully understand the risk-benefit profile of cataract surgery.
Ask your ophthalmologist to walk you through which complications are most relevant given your specific eye health. Knowing the likelihood of each issue, even when risks are low overall, helps set realistic expectations before surgery day.
How Likely Is Posterior Capsule Opacification and How Is It Treated?
Posterior capsule opacification is the most likely long-term complication, though its occurrence varies widely depending on lens material, surgical technique, and individual healing response. PCO develops when residual lens epithelial cells migrate and proliferate across the posterior capsule, gradually clouding vision months or years after the original procedure.
Treatment involves a YAG laser capsulotomy, a quick, painless outpatient procedure. The laser creates a small opening in the opacified capsule, restoring clear vision almost immediately. Most patients notice improvement within hours. Because YAG capsulotomy is well established and carries minimal risk, PCO is considered more of an expected follow-up event than a serious complication. Your surgeon should explain whether the IOL chosen for your procedure has design features that may reduce PCO incidence over time.
What Happens if Your Refractive Outcome Is Not as Expected?
A refractive outcome that is not as expected means your post-surgical vision does not match the target prescription your surgeon planned. This is sometimes called a “refractive surprise,” and while uncommon with modern biometry, it can occur due to measurement variability, unusual corneal healing, or lens positioning.
Your ophthalmologist may recommend several corrective options:
- Prescription glasses or contact lenses to address the residual error.
- A lens exchange procedure if the refractive miss is significant and detected early.
- A secondary enhancement, such as LASIK or PRK, once the eye has fully stabilized.
Ask your surgeon before the procedure what their threshold is for considering a corrective intervention and how frequently refractive surprises occur in their practice. This conversation often reveals both the surgeon’s experience level and their commitment to achieving your visual goals.
How Does Your Surgeon Handle Rare but Serious Complications?
Your surgeon handles rare but serious complications through established emergency protocols, immediate access to specialized equipment, and a clear plan communicated before surgery. Complications such as endophthalmitis, retinal detachment, or significant intraocular hemorrhage are uncommon, yet they require swift, decisive intervention.
Key questions to ask include:
- What is your protocol if an infection develops in the first 48 hours?
- Do you have access to a retinal specialist if a referral becomes necessary?
- Where would emergency treatment take place, and how quickly can it be arranged?
A surgeon who answers these questions openly and in detail demonstrates the kind of preparedness that reflects strong clinical judgment. Hesitation or vagueness on emergency planning can be a meaningful signal during your consultation evaluation.
Understanding your surgeon’s approach to worst-case scenarios provides confidence that extends well beyond the operating room.
What Questions Should You Ask About Recovery and Aftercare?
The questions you should ask about recovery and aftercare cover first-week expectations, activity timelines, prescribed medications, and follow-up scheduling.
What Can You Expect in the First Week After Surgery?
You can expect mild discomfort, light sensitivity, and gradually improving vision in the first week after surgery. Most patients notice clearer sight within a few days, though some blurriness and fluctuation is normal as the eye heals. Your surgeon may recommend wearing a protective shield while sleeping to prevent accidental rubbing or pressure on the eye.
Common first-week experiences include:
- Mild itching or a gritty sensation in the treated eye
- Sensitivity to bright lights
- Watery eyes or slight discharge
- Gradual sharpening of vision over several days
Strenuous activity, heavy lifting, and swimming should be avoided during this initial healing window. From a practical standpoint, planning ahead for someone to assist with daily tasks during the first 48 hours can make the recovery period significantly smoother for most patients.
When Can You Safely Return to Driving and Daily Activities?
You can safely return to driving and daily activities once your surgeon confirms that your visual acuity meets the legal standard, which typically occurs within a few days to one week after surgery. Light tasks around the home can often resume within 24 to 48 hours, while more demanding activities may require a longer waiting period.
This timeline matters because cataract surgery is considered medically necessary when the cataract limits a patient’s ability to perform activities of daily living. According to AARP’s coverage of Medicare policy, Medicare covers cataract surgery when the cataract causes symptomatic impairment of visual function that limits activities such as reading, driving, or vocational needs. Restoring the ability to perform these specific activities safely is a core recovery milestone, so your surgeon’s clearance before resuming driving is essential.
Which Medications and Eye Drops Will You Need After Surgery?
The medications and eye drops you will need after surgery typically include a combination of antibiotic, anti-inflammatory, and steroid drops prescribed on a structured schedule. According to the Cleveland Clinic, postoperative protocols involve this multi-drop regimen, though some modern centers now offer “dropless” surgery using intraocular medications injected at the time of the procedure.
Your surgeon should explain:
- The specific drop schedule and duration for each medication
- Proper technique for administering eye drops without touching the eye
- Whether you are a candidate for a dropless surgical approach
- Any potential side effects to watch for
Patients increasingly want to know whether they will need glasses for reading after surgery. This is a reasonable question to raise during your aftercare discussion, as the answer depends on the IOL type selected and your individual healing response.
How Many Follow-Up Visits Are Typically Required?
The number of follow-up visits typically required after cataract surgery ranges from three to four appointments over the first month. A standard post-operative schedule often includes visits at one day, one week, and one month after the procedure, though your surgeon may adjust this based on your healing progress and any pre-existing conditions.
These visits allow your ophthalmologist to:
- Monitor intraocular pressure and check for inflammation
- Assess visual acuity improvements
- Evaluate the IOL position and stability
- Update your glasses prescription once healing stabilizes
Missing follow-up appointments can delay the detection of treatable complications. Even when recovery feels entirely smooth, keeping every scheduled visit remains one of the simplest ways to protect your surgical outcome.
With recovery expectations established, understanding the financial side of cataract surgery helps you plan with confidence.
What Should You Ask About Costs and Insurance Coverage?
You should ask about costs and insurance coverage to understand what your plan pays for standard cataract surgery, what you owe for premium lens upgrades, and whether financing can bridge the gap.
Does Insurance or Medicare Cover Standard Cataract Surgery?
Insurance and Medicare generally cover standard cataract surgery when it is deemed medically necessary. Medicare Part B classifies cataract extraction as a covered procedure when the cataract causes functional visual impairment that limits activities of daily living, such as reading or driving, and cannot be corrected with glasses alone.
For 2026, the Medicare Part B deductible is $283. After meeting this deductible, Medicare pays 80% of the approved amount, leaving the patient responsible for the remaining 20% coinsurance. A Medigap or Medicare Supplement plan may cover part or all of that remaining balance.
Most private insurance plans follow similar medical necessity criteria, though specific deductibles and copay structures vary by carrier. According to the 2026 Medicare Physician Fee Schedule, surgeon reimbursement for standard cataract surgery (CPT 66984) reflects an approximate 11% reduction compared to prior years, a shift worth discussing with your surgical team regarding facility fees and billing. Always request a pre-authorization and itemized cost estimate before scheduling.
What Out-of-Pocket Costs Apply When Choosing a Premium IOL?
Out-of-pocket costs for a premium IOL cover the price difference between a standard monofocal lens and the advanced technology lens you select. Medicare and most private insurers consider multifocal, extended depth of focus, and toric IOLs to be elective enhancements. The insurer pays the amount it would have covered for a standard lens implant; the patient pays everything above that baseline.
These additional fees typically include:
- The upgraded lens itself
- Any specialized diagnostic testing required for premium IOL selection, such as optical biometry or topography
- Potential laser-assisted surgical fees if femtosecond technology is used alongside the premium lens
Costs for premium IOLs can range widely depending on lens type and practice location. Your surgeon’s office should provide a written breakdown separating the insurance-covered portion from the patient-responsibility portion before you commit. This transparency is especially important because the financial component is one of the most common sources of post-surgical dissatisfaction when expectations are not set clearly upfront.
Are Financing Options Available for Upgraded Lens Technology?
Financing options for upgraded lens technology are available at many ophthalmology practices. Because premium IOL costs are considered elective, they fall outside standard insurance coverage, and practices commonly offer structured payment solutions to make these upgrades accessible.
Common financing arrangements include:
- Medical credit lines, such as CareCredit or Alphaeon, which may offer promotional interest-free periods
- In-house payment plans that divide the patient-responsibility balance across several months
- Health Savings Account (HSA) or Flexible Spending Account (FSA) funds, which can be applied to qualified out-of-pocket surgical expenses
Ask your surgeon’s billing coordinator which options the practice accepts and whether any promotional terms apply. Confirming financing details before your procedure date prevents unexpected financial stress during recovery.
Understanding the full financial picture, from insurance coverage to premium lens fees to available payment plans, helps you make a confident, well-informed decision about your cataract surgery.
How Should You Evaluate Your Cataract Surgeon’s Experience?
You should evaluate your cataract surgeon’s experience by verifying credentials, surgical volume, and lens-specific expertise. The following subsections cover board certifications, procedure counts, and IOL familiarity.
What Credentials and Board Certifications Should You Look For?
The credentials and board certifications you should look for include board certification by the American Board of Ophthalmology (ABO) and fellowship training in a relevant subspecialty. ABO certification requires passing rigorous written and oral examinations, with recertification required every ten years to confirm ongoing competency.
Beyond board certification, fellowship status from the American Academy of Ophthalmology (AAO) signals additional professional recognition. AAO Fellowship (FAAO) status indicates that a surgeon is a member in good standing who has met specific educational and clinical practice standards recognized by the Academy, according to the AAO.
You may also want to confirm whether the surgeon completed a fellowship in anterior segment surgery or a cornea/refractive subspecialty. These focused training programs build deeper expertise in lens-based procedures. In practice, a surgeon who holds both ABO certification and a relevant subspecialty fellowship typically brings the strongest clinical foundation to cataract cases.
How Many Cataract Procedures Has the Surgeon Performed?
The number of cataract procedures a surgeon has performed is one of the most practical indicators of technical proficiency. Higher surgical volume is generally associated with greater consistency, faster operative times, and lower complication rates.
When evaluating volume, consider asking these specific questions:
- How many cataract surgeries does the surgeon perform per week or per year?
- How many total procedures has the surgeon completed over the course of their career?
- What is the surgeon’s personal complication rate compared to national benchmarks?
A surgeon who routinely performs several hundred procedures annually has likely encountered a wide range of anatomical variations and intraoperative challenges. This accumulated experience can be especially important for patients with dense cataracts, small pupils, or other complicating factors. Do not hesitate to ask directly; experienced surgeons are typically comfortable sharing these numbers.
Does the Surgeon Have Experience With the Specific IOL You Want?
The surgeon’s experience with the specific IOL you want directly influences your visual outcome. Each intraocular lens platform, whether monofocal, toric, multifocal, extended depth of focus, or light adjustable, requires distinct surgical techniques and postoperative management protocols.
Consider asking the following:
- How many implantations of this particular IOL model has the surgeon performed?
- What patient satisfaction and visual outcomes has the surgeon observed with this lens?
- Does the surgeon have access to the latest lens platforms and sizing technology?
A surgeon who frequently implants a specific lens develops refined skills in patient selection, precise lens positioning, and managing any lens-specific visual side effects. For premium lenses in particular, this familiarity often makes the difference between a good result and an exceptional one.
Understanding your surgeon’s qualifications and experience sets a strong foundation before seeking additional perspectives.
What Questions Should You Bring to a Second Opinion Consultation?
The questions you should bring to a second opinion consultation focus on confirming your diagnosis, validating the recommended surgical approach, and comparing intraocular lens recommendations between surgeons.
A second opinion can be particularly valuable when the first surgeon’s IOL recommendation feels unclear, when you have complex eye conditions alongside cataracts, or when the proposed treatment plan involves premium technology with significant out-of-pocket costs. Preparing specific, targeted questions ensures the consulting ophthalmologist can provide meaningful feedback rather than simply repeating baseline tests.
Key questions to bring include:
- Do you agree with the cataract staging and timeline for surgery recommended by my first surgeon?
- Would you recommend the same intraocular lens type, or do you see a better option for my visual goals and eye anatomy?
- Are there any additional diagnostic measurements you would perform before confirming my surgical plan?
- Do my existing eye conditions, such as astigmatism, dry eye, or prior refractive surgery, change your recommended approach?
- How does your preferred surgical technique compare to what was initially proposed?
When seeking a second opinion, bring copies of your diagnostic records, including biometry readings and OCT scans, so the consulting surgeon can evaluate your case without unnecessary duplicate testing. Differences in IOL recommendations between two qualified surgeons often reflect legitimate variations in clinical philosophy rather than errors. The goal is not to find the “right” answer but to understand the reasoning behind each recommendation so you can make a confident, informed decision. With your questions prepared, surgeon-led educational resources can further strengthen your understanding before the consultation.
How Can Educational Resources Help You Prepare for Your Cataract Consultation?
Educational resources can help you prepare for your cataract consultation by providing clinically accurate, unbiased information that builds confidence before you meet your ophthalmologist. The sections below cover how Eye Surgery Today supports IOL decision-making and the essential takeaways for your appointment.
Can Eye Surgery Today Help You Understand Your IOL Choices Before Your Appointment?
Yes, Eye Surgery Today can help you understand your IOL choices before your appointment. As an education platform founded by nationally recognized key opinion leaders in ophthalmology, Eye Surgery Today translates complex lens technology into clear, accessible language. Eye Surgery Today publishes comprehensive guides covering monofocal, multifocal, extended depth of focus, toric, and light adjustable lens options, so patients can arrive at their consultation already familiar with the terminology and trade-offs their surgeon will discuss.
This kind of preparation matters because IOL selection directly shapes post-surgical visual outcomes. When patients understand the basic differences between lens categories beforehand, the consultation itself becomes a more productive, two-way conversation rather than an overwhelming information dump. Eye Surgery Today’s educational articles, surgeon profiles, and video resources provide the foundation patients need to ask focused, informed questions about which lens best fits their lifestyle and visual goals.
What Are the Key Takeaways About Questions to Ask at Your Cataract Consultation?
The key takeaways about questions to ask at your cataract consultation are:
- Understand your diagnosis thoroughly. Ask about your specific cataract type, its severity, and whether other eye conditions contribute to your vision loss.
- Clarify your surgical candidacy. Discuss how existing health conditions, previous refractive surgeries, or concurrent eye diseases may influence your surgical plan and timing.
- Explore every IOL option. Request a clear comparison of standard monofocal, multifocal, EDOF, toric, and light adjustable lenses, including how each aligns with your daily visual needs.
- Ask about the procedure itself. Understand the surgical technique your surgeon recommends, the reasoning behind it, and what anesthesia will be used.
- Know the risks and how they are managed. Ask specifically about common complications and your surgeon’s protocol for handling unexpected outcomes.
- Plan for recovery and costs. Confirm the postoperative medication regimen, follow-up schedule, activity restrictions, and any out-of-pocket expenses for premium lens upgrades.
Arriving with these questions organized gives you the structure to cover every critical topic during a consultation that may feel rushed. Eye Surgery Today’s educational guides are designed to help patients build exactly this kind of preparation, turning uncertainty into informed confidence before surgery day.
