 Simulating your vision plan with contact lenses before surgery is a preoperative approach that uses temporary contact lenses to preview how different intraocular lens (IOL) implants may affect your sight before committing to a permanent surgical correction. This process allows patients considering cataract surgery or refractive lens exchange to experience the optical characteristics of various IOL types in real-world conditions.
Simulating your vision plan with contact lenses before surgery is a preoperative approach that uses temporary contact lenses to preview how different intraocular lens (IOL) implants may affect your sight before committing to a permanent surgical correction. This process allows patients considering cataract surgery or refractive lens exchange to experience the optical characteristics of various IOL types in real-world conditions.
We cover the clinical purpose behind contact lens simulation, the specific IOL types you can preview, what happens during a simulation appointment, candidacy and limitations, monovision decision-making, and how expert surgical education supports the process.
Contact lens simulation works by fitting trial lenses calibrated to approximate monofocal, multifocal, extended depth-of-focus (EDOF), and monovision IOL profiles. Each lens type produces distinct visual trade-offs; for example, multifocal trials may reveal reduced spectacle dependence alongside potential halos, while monovision trials test whether your brain can comfortably adapt to intentionally different focus between your two eyes.
The simulation appointment itself involves baseline measurements including refraction, keratometry, biometry, and ocular surface screening, followed by a structured wear period of one to two weeks. During this time, patients evaluate clarity across daily tasks like driving, reading, and screen work to generate concrete feedback for their surgeon.
Not every patient requires a simulation, and the process carries inherent limitations. Contact lenses sit on the corneal surface rather than inside the eye, so they cannot replicate internal optical phenomena like dysphotopsia or the full neuroadaptation process. Undetected dry eye or ocular surface disease may also reduce simulation accuracy.
Combining hands-on trial results with targeted questions for your surgeon and reliable, physician-led educational resources can help strengthen your confidence and support a well-informed lens selection.
What Does It Mean to Simulate Vision with Contact Lenses Before Eye Surgery?
Simulating vision with contact lenses before eye surgery means using temporary contact lenses to preview how different intraocular lens (IOL) options may affect your sight before committing to a permanent implant. This preoperative approach allows patients considering cataract surgery or refractive lens exchange to experience the visual characteristics of monofocal, multifocal, extended depth-of-focus (EDOF), and monovision corrections in real-world conditions.
Rather than relying solely on clinical descriptions or digital charts, a contact lens simulation places the anticipated optical outcome directly on your eyes. You can then evaluate clarity at various distances, notice any visual trade-offs, and assess comfort during everyday tasks. According to a 2025 review published in Biomedical Optics Express, visual simulators of IOLs are advanced optical and computational instruments designed to aid ophthalmologists and patients in the preoperative assessment and selection of the most suitable IOL for cataract surgery or refractive lens exchange. Contact lens trials represent one of the most accessible forms of this simulation, offering a tangible, patient-centered preview that digital tools alone cannot fully replicate.
The core purpose is informed decision-making. When a patient wears trial lenses calibrated to approximate a specific IOL design, the experience bridges the gap between abstract surgical planning and lived visual perception. This process can promote a stronger sense of agency, because a mismatch between expectations and outcomes has been shown to foster regret. Effective preoperative simulation helps patients feel cognitive ownership over their lens choice, reducing uncertainty and strengthening confidence heading into the operating room.
For ophthalmologists, the simulation also serves as a clinical feedback tool. Patient responses during the trial period provide valuable data that complements biometry, keratometry, and refraction measurements. This combination of subjective experience and objective diagnostics supports individualized surgical planning, which is considered essential for optimizing postoperative satisfaction. Understanding what this simulation involves, and what it can realistically show you, is the first step toward making a confident, well-informed vision decision.
Why Would Your Surgeon Recommend a Contact Lens Trial Before Surgery?
Your surgeon would recommend a contact lens trial before surgery to help you experience potential visual outcomes before committing to a permanent lens implant. This preoperative step supports informed consent, manages expectations, and identifies the best IOL strategy for your lifestyle.
A contact lens trial before cataract surgery or refractive lens exchange serves several important purposes. First, it transforms an abstract decision into a concrete, lived experience. Rather than choosing between monofocal, multifocal, or monovision IOLs based on descriptions alone, patients can test how each correction strategy feels during everyday tasks. This real-world evaluation helps surgeons and patients collaborate on a vision plan that aligns with individual visual demands.
The trial also strengthens the informed consent process. According to the British Medical Journal, valid consent requires that the patient be competent to take the particular decision, have received sufficient information to make it, and act of their own free will. A contact lens simulation directly addresses the second requirement by giving patients experiential knowledge of what each lens option may deliver, rather than relying solely on verbal explanations or printed charts.
Beyond consent, expectation management plays a critical role in surgical satisfaction. A mismatch between expectations and outcomes can create a perceived loss of control, which, as discussed at the 2024 ESCRS Meeting, may foster regret. Effective preoperative simulation promotes a sense of agency and cognitive ownership over the decision. When patients have already lived with a vision correction strategy for days or weeks, they enter surgery with realistic expectations, reducing the likelihood of postoperative dissatisfaction.
Surgeons also use trial results diagnostically. The patient’s feedback on comfort, visual clarity at different distances, and tolerance of optical trade-offs, such as halos or reduced contrast, informs the final IOL selection. For patients considering monovision or multifocal correction, this step can reveal neuroadaptation challenges that would otherwise surface only after an irreversible procedure.
In practice, a surgeon’s recommendation for a contact lens trial reflects a commitment to individualized decision-making, prioritizing each patient’s functional needs over a one-size-fits-all approach. Understanding how the trial connects to specific lens implant options is the next step in building your vision plan.
How Does a Contact Lens Simulation Help You Choose the Right Lens Implant?
A contact lens simulation helps you choose the right lens implant by letting you experience different optical profiles before committing to surgery. The following subsections cover how trials replicate monofocal, multifocal, monovision, and extended depth of focus IOL outcomes.
How Can a Contact Lens Trial Simulate Monofocal IOL Outcomes?
A contact lens trial can simulate monofocal IOL outcomes by fitting a single-vision contact lens set to your target distance refraction, typically optimized for clear far vision. Wearing this lens during everyday tasks reveals what crisp distance clarity feels like while also exposing the reading glasses dependence that accompanies a monofocal implant.
Because monofocal IOLs correct one focal point, the trial lens intentionally leaves near and intermediate ranges uncorrected. This gives patients a realistic preview of activities like reading a phone screen or viewing a computer monitor without additional correction. From a practical standpoint, even a brief trial period makes the trade-off between sharp distance acuity and near-vision limitation far more tangible than any verbal explanation alone.
How Can a Contact Lens Trial Simulate Multifocal IOL Outcomes?
A contact lens trial can simulate multifocal IOL outcomes by using a multifocal contact lens that distributes light across multiple focal points, allowing simultaneous distance and near vision in the same eye. Patients experience the reduced spectacle dependence that multifocal implants offer, along with potential visual compromises such as halos or mild contrast reduction.
According to a study published in the Journal of Cataract and Refractive Surgery, multifocal IOL insertion was associated with less spectacle dependence compared to mini-monovision, though both strategies provided excellent refractive outcomes for distance vision. A contact lens trial replicates this dynamic by letting patients assess whether the added near function outweighs any perceived optical side effects during real-world activities. Patients who tolerate the multifocal contact lens well are often strong candidates for a multifocal implant, while those bothered by visual disturbances can explore alternatives before surgery.
How Can a Contact Lens Trial Simulate Monovision Correction?
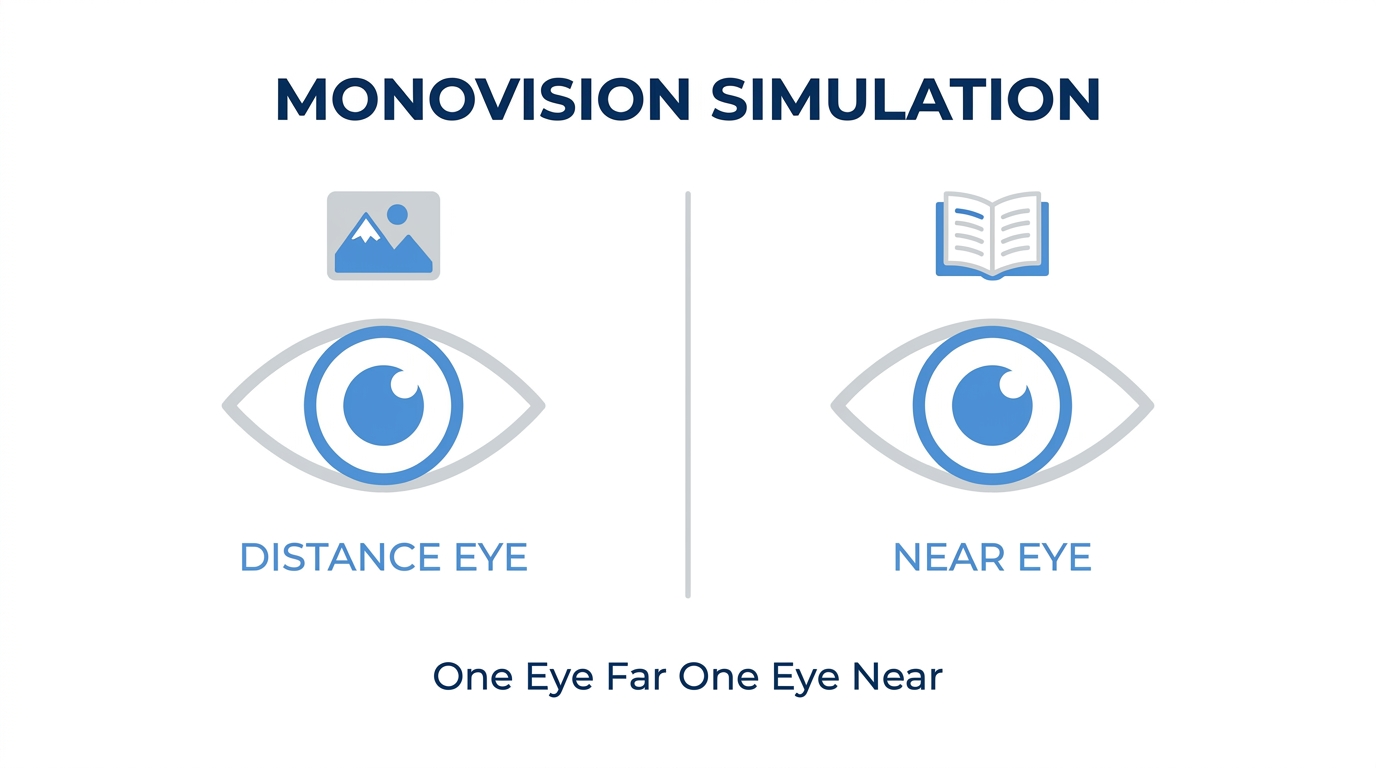
A contact lens trial can simulate monovision correction by fitting one eye with a contact lens optimized for distance and the other with a lens targeted for near vision. This intentional imbalance between the two eyes mimics the blended vision strategy used in monovision IOL surgery.
The brain must learn to suppress the slightly blurred image from one eye depending on the task, a process called neuroadaptation. During the trial period, patients evaluate depth perception, comfort while driving, and ease of reading. Some individuals adapt quickly and find the trade-off acceptable, while others notice persistent imbalance or reduced stereopsis that signals monovision may not suit them. Testing this approach with removable contact lenses before permanent surgical correction is one of the most reliable ways to predict patient satisfaction.
How Can a Contact Lens Trial Simulate Extended Depth of Focus Lenses?
A contact lens trial can simulate extended depth of focus lenses by using specially designed contact lenses that elongate the focal range rather than splitting light into discrete near and far zones. EDOF lenses aim to provide continuous vision from distance through intermediate, reducing the abrupt optical transitions associated with traditional multifocal designs.
According to a 2025 review in Biomedical Optics Express, visual simulators incorporate deformable mirrors, spatial light modulators, and optotunable lenses to replicate monofocal, multifocal, and EDOF IOL profiles, including newer designs aimed at improving contrast sensitivity and expanding depth of focus. While contact lens trials cannot perfectly replicate every EDOF optical element, they offer patients a meaningful preview of the smoother visual transition and improved intermediate clarity these implants provide. For patients who need functional computer-distance vision without the halo profile of a multifocal, an EDOF simulation trial is particularly informative.
With each lens type tested through contact lens simulation, the next step is understanding what happens during the simulation appointment itself.
What Happens During a Contact Lens Vision Simulation Appointment?
A contact lens vision simulation appointment involves precise eye measurements, fitting of trial lenses, and a real-world testing period. The sections below cover initial measurements, recommended wear time, and daily tasks to evaluate.
What Measurements Does Your Eye Doctor Take First?
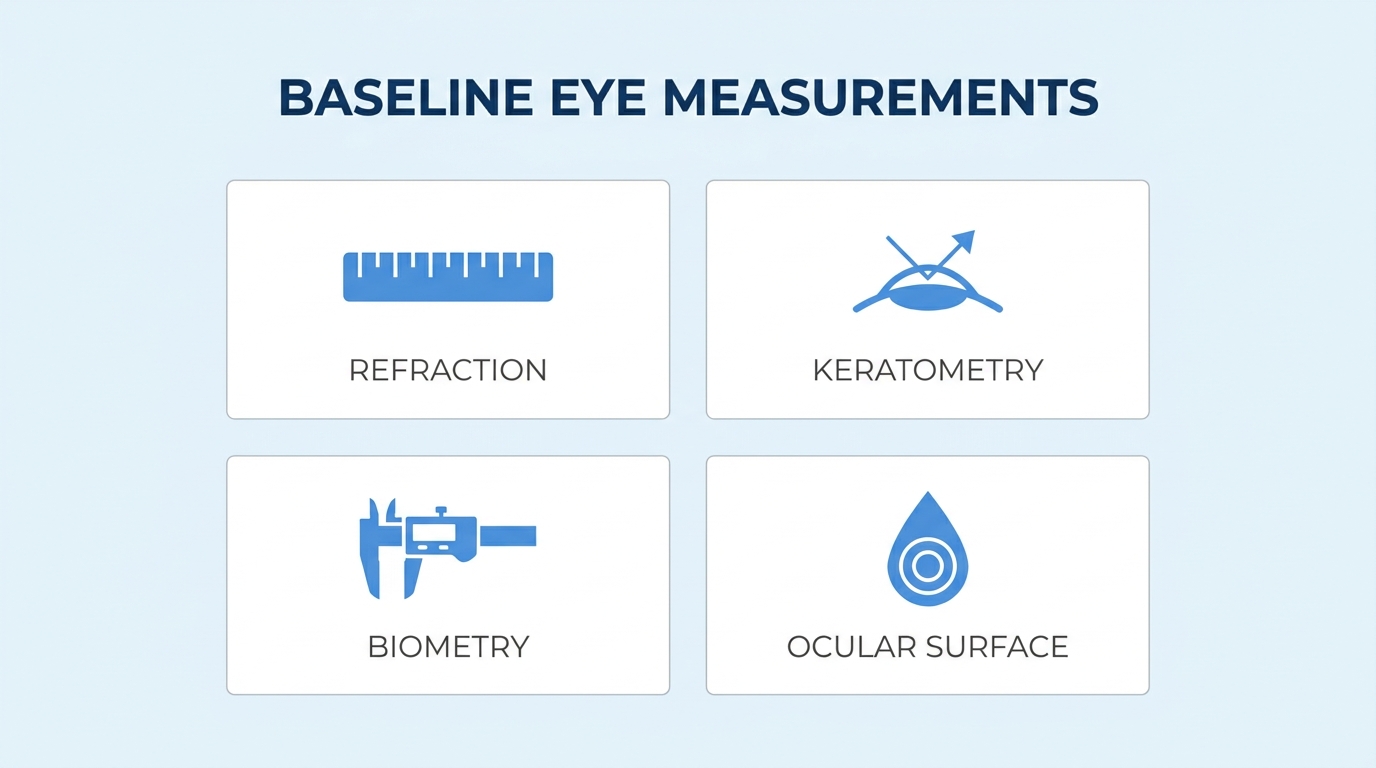
Your eye doctor takes several baseline measurements first to ensure the trial lenses accurately replicate your planned surgical outcome. These measurements establish the optical starting point for your simulation.
Key measurements typically include:
- Refraction to determine your current prescription and the correction needed for each eye.
- Keratometry to map corneal curvature, which affects how a contact lens sits and performs.
- Biometry to measure axial length and other dimensions used in IOL power calculations.
- Ocular surface assessment to screen for dry eye disease or other conditions that could compromise simulation accuracy.
According to a 2019 study published in the Journal of Cataract and Refractive Surgery, the impact of dry eye disease and ocular surface disease on topography, biometry, and keratometry is one of the major causes of disappointing postoperative outcomes. Addressing these factors before fitting trial lenses helps ensure the simulation reflects realistic surgical results. Without accurate baseline data, even a well-designed contact lens trial can mislead decision-making.
How Long Should You Wear the Trial Lenses Before Deciding?
You should wear the trial lenses for at least several days, and often one to two weeks, before deciding on your surgical lens choice. A single office visit cannot capture how your brain adapts to a new visual configuration across varied lighting and tasks.
According to SimVis Gekko (2EyesVision), a typical evaluation using a binocular simulator can take an optometrist at least 20 minutes, involving replication of through-focus performance of various IOLs to rate satisfaction with near and distance visual acuity. However, real-world adaptation, particularly with monovision or multifocal designs, requires neuroadaptation that unfolds over days. Rushing the trial period risks basing a permanent surgical decision on an incomplete experience.
What Daily Tasks Should You Test During the Simulation Period?
The daily tasks you should test during the simulation period are the activities most important to your lifestyle and visual demands. Contact lens trials allow patients to evaluate how their vision feels during real-world activities such as playing badminton, attending orchestra rehearsals, chairing a meeting, and driving at night, as noted by Brendan Cummings, MBBChBAO, FRCSI(Ophth), FEBO, FWCRS.
Priority tasks to evaluate include:
- The daily tasks you should test during the simulation period are the activities most important to your lifestyle and visual demands. Contact lens trials allow patients to “evaluate how their vision feels during real-world activities such as playing badminton, attending orchestra rehearsals, chairing a meeting, and driving at night,” Brendan Cummings, MBBChBAO, FRCSI(Ophth), FEBO, FWCRS, notes.
Documenting your experience with each activity gives your surgeon concrete feedback for refining the final IOL selection. With your simulation results in hand, the next step is determining whether you are a strong candidate for this preoperative approach.
Who Is a Good Candidate for a Contact Lens Simulation Before Surgery?
A good candidate for a contact lens simulation before surgery is any patient considering a premium or specialty intraocular lens who wants to preview how different vision correction strategies feel in daily life. Several patient profiles benefit most from this preoperative step.
- Cataract surgery patients choosing between IOL types. Anyone weighing monofocal, multifocal, extended depth-of-focus, or monovision lenses can use a contact lens trial to compare real-world visual outcomes before committing to a permanent implant. Understanding the long-term implications, including the possibility of an intraocular lens exchange, helps patients make fully informed choices.
- Patients with strong spectacle independence goals. Those who want to reduce or eliminate glasses after surgery benefit from experiencing how each lens strategy handles near, intermediate, and distance tasks.
- Monovision candidates uncertain about adaptation. Patients curious about blended vision need to test whether their brain can comfortably suppress one eye’s blur during activities like reading and driving.
- Patients with high visual demands. Professionals, musicians, or athletes whose work requires precise vision at specific distances gain the most from a structured trial period.
- Anxious or detail-oriented patients. Individuals who feel uncertain about surgical outcomes often gain confidence when they can physically experience a vision plan rather than relying solely on verbal descriptions.
According to a 2024 report presented at the ESCRS Meeting, a mismatch between expectations and outcomes can create a perceived loss of control among patients, which may foster regret; effective preoperative simulation promotes a sense of agency and cognitive ownership. This finding highlights why candidates who struggle with decision-making or fear postoperative dissatisfaction are especially well suited for a trial.
Not every patient requires a simulation, however. Those opting for a standard monofocal lens targeting clear distance vision, with a plan to wear reading glasses, may find the process unnecessary. Patients with active ocular surface disease or unstable refraction should address those conditions first, since compromised tear film can distort contact lens performance and reduce simulation accuracy. In clinical practice, the patients who gain the most value from this step are those facing a genuine choice between two or more lens strategies, where the “right” answer depends on personal lifestyle priorities rather than a single clinical measurement.
Understanding candidacy helps set expectations, but recognizing the limitations of contact lens simulation is equally important.
What Are the Potential Limitations of Simulating Surgery with Contact Lenses?
The potential limitations of simulating surgery with contact lenses include differences in optical performance between external lenses and implanted IOLs, visual phenomena that contact lenses cannot replicate, and ocular surface conditions that may reduce simulation accuracy.
Can Contact Lenses Perfectly Replicate Intraocular Lens Performance?
No, contact lenses cannot perfectly replicate intraocular lens performance. A contact lens sits on the corneal surface, while an IOL is implanted inside the eye, replacing the natural crystalline lens. This fundamental difference in optical position affects how light bends, scatters, and focuses on the retina.
Key performance gaps include:
- Contact lenses cannot reproduce the fixed internal optics of an IOL, which interacts directly with the eye’s internal structures.
- Multifocal and EDOF IOL designs split or extend light in ways that external lenses approximate but do not match precisely.
- Contrast sensitivity, a critical measure of visual quality, may differ between a contact lens trial and actual postoperative results with an implanted lens.
According to Rayner Intraocular Lenses Limited, monovision with the RayOne EMV IOL provided high patient satisfaction, with preserved contrast sensitivity, good distance vision, and functional intermediate vision. These nuanced optical outcomes are difficult to replicate fully with a surface contact lens. For this reason, a contact lens trial should be viewed as a practical preview rather than an exact prediction of surgical results.
What Visual Factors Can a Contact Lens Trial Not Simulate?
The visual factors a contact lens trial cannot simulate include internal optical phenomena unique to intraocular lenses. Because IOLs sit inside the eye and interact with the pupil, capsular bag, and vitreous, they produce visual effects that no external lens can recreate.
Factors beyond the reach of contact lens simulation include:
- Dysphotopsia, such as halos, glare, and starbursts, which arise from light diffraction at the IOL edge inside the eye.
- Neuroadaptation, the brain’s gradual adjustment to a new internal optical system over weeks or months after surgery.
- Internal higher-order aberrations introduced by the IOL’s interaction with the eye’s unique biometry and keratometry readings.
Patients should understand that while a contact lens trial reveals general functional comfort with a vision strategy, it cannot preview every sensory experience of living with an implanted lens. Discussing these gaps with your ophthalmologist helps set realistic expectations before committing to a specific IOL.
How Might Tear Film or Dry Eye Affect Simulation Accuracy?
Tear film instability or dry eye may significantly affect simulation accuracy during a contact lens trial. A contact lens relies on a smooth, stable tear film to maintain consistent optics. When the ocular surface is compromised, the simulation may misrepresent the visual quality a patient would actually achieve after IOL implantation.
According to an American Society of Cataract and Refractive Surgery (ASCRS) clinical report, upwards of 60% of routine cataract patients were asymptomatic for dry eye disease, yet 50% had central corneal staining, and over 50% of asymptomatic patients had an abnormal tear osmolarity or MMP-9 level. This means many patients entering a contact lens trial carry undetected ocular surface disease that can distort results.
Dry eye and ocular surface disease may affect simulation in several ways:
- Fluctuating vision during the trial due to an unstable tear film over the contact lens.
- Inaccurate refraction measurements that inform lens selection.
- Discomfort that shortens wear time and limits real-world testing.
Addressing ocular surface health before beginning any contact lens simulation helps ensure the trial reflects true optical potential rather than a compromised baseline. With these limitations understood, realistic expectations become the foundation for a more productive conversation with your surgeon.
How Does Monovision Simulation Help You Decide About Blended Vision Surgery?
Monovision simulation helps you decide about blended vision surgery by letting you experience the intentional difference in focus between your two eyes before committing to a permanent lens implant. The following subsections cover what to expect during the trial, how long neuroadaptation typically takes, and which warning signs may indicate monovision is not the right fit.
What Should You Expect During a Monovision Contact Lens Trial?
During a monovision contact lens trial, you should expect to wear one contact lens set for distance vision and the other for near vision, then evaluate how this split-focus arrangement feels across your normal routine. Your eye doctor will prescribe a specific lens power for each eye based on your refraction and biometry measurements.
The real value of the trial emerges outside the clinic. According to ophthalmologist Brendan Cummings, MBBChBAO, FRCSI(Ophth), contact lens trials allow patients to evaluate how their vision feels during real-world activities such as playing badminton, attending orchestra rehearsals, chairing a meeting, and driving at night. Testing under varied lighting conditions and at different working distances reveals whether the monovision balance suits your lifestyle. Patients who rely heavily on sharp binocular depth perception, for instance, often notice the compromise more acutely during these practical tasks than during a brief office assessment.
During a monovision contact lens trial, you should expect to wear one contact lens set for distance vision and the other for near vision, then evaluate how this split-focus arrangement feels across your normal routine. Your eye doctor will prescribe a specific lens power for each eye based on your refraction and biometry measurements.
The real value of the trial emerges outside the clinic. According to ophthalmologist Brendan Cummings, MBBChBAO, FRCSI(Ophth), contact lens trials allow patients to “evaluate how their vision feels during real-world activities such as playing badminton, attending orchestra rehearsals, chairing a meeting, and driving at night.” Testing under varied lighting conditions and at different working distances reveals whether the monovision balance suits your lifestyle. Patients who rely heavily on sharp binocular depth perception, for instance, often notice the compromise more acutely during these practical tasks than during a brief office assessment.
How Long Does It Take Your Brain to Adapt to Monovision Simulation?
It typically takes your brain one to two weeks to adapt to monovision simulation, though full neuroadaptation can require up to four weeks for some individuals. During this period, the visual cortex gradually learns to suppress the slightly blurred image from each eye depending on the viewing distance, a process known as neuroadaptation.
Most patients notice the imbalance feels less pronounced after the first few days. By the end of the second week, the brain has usually begun prioritizing the dominant eye for distance and the non-dominant eye for near tasks without conscious effort. Rushing a decision before this adaptation window closes can lead to a premature rejection of an approach that might have worked well. For patients who still feel visually uncomfortable or disoriented after a full month of consistent wear, that sustained difficulty is itself a meaningful clinical finding worth discussing with your ophthalmologist.
What Signs Suggest Monovision May Not Be Right for You?
The signs that suggest monovision may not be right for you include persistent visual discomfort, difficulty with depth perception, and ongoing headaches or eye strain that do not resolve during the adaptation period. Specific warning signs to watch for include:
- Continued difficulty judging distances when driving, especially at night.
- Frequent headaches or a sensation of eye fatigue after routine near tasks.
- Persistent double vision or shadowing that does not diminish over several weeks.
- Significant dissatisfaction with intermediate-distance clarity, such as reading a computer screen.
- A strong sense of visual imbalance that interferes with work or recreational activities.
If any of these symptoms persist beyond the typical neuroadaptation window, monovision correction may not align with your visual demands. In such cases, your surgeon may recommend alternative lens options, such as multifocal or extended depth-of-focus IOLs, that distribute focus across multiple distances without relying on interocular suppression. Honest feedback from the simulation trial gives your ophthalmologist the clinical evidence needed to guide you toward a better-suited surgical plan.
What Questions Should You Ask Your Surgeon About Your Simulation Results?
The questions you should ask your surgeon about your simulation results focus on how well the trial reflects your expected surgical outcome, which IOL best matches your lifestyle, and whether any factors could change the final result.
- “Which IOL type best matches what I experienced during my contact lens trial?” Your surgeon can compare your simulation experience with the optical profile of monofocal, multifocal, EDOF, or monovision IOLs to identify the closest match.
- “Will I still need glasses after surgery?“ According to Griffey Eye Care & Laser Center, this ranks among the most common patient questions before cataract surgery, and your simulation results give your surgeon concrete data to answer it.
- “How closely does my contact lens trial replicate actual IOL performance?” Contact lenses cannot perfectly simulate factors like dysphotopsia, neuroadaptation, or internal lens optics, so understanding the gap between trial and outcome helps set realistic expectations.
- “Could dry eye or ocular surface disease affect my surgical results differently than my simulation?” Tear film instability can distort simulation accuracy and, separately, influence postoperative outcomes through its impact on biometry and keratometry measurements.
- “What happens if I’m unhappy with the vision outcome after surgery?” A mismatch between expectations and outcomes can foster regret, so discussing contingency plans before surgery promotes a stronger sense of agency in your decision.
- “How long will neuroadaptation take after surgery compared to my trial period?” Your brain adapts differently to a permanent IOL than to removable contact lenses, and your surgeon can outline a realistic adaptation timeline.
Asking these targeted questions transforms your simulation data into a shared decision-making tool. With your simulation concerns addressed, understanding the risks of skipping a contact lens trial altogether adds another layer to your preparation.
What Are the Possible Risks of Skipping a Contact Lens Trial Before Surgery?
The possible risks of skipping a contact lens trial before surgery include mismatched expectations, reduced informed consent, and postoperative dissatisfaction with your chosen lens implant. Patients should also be aware of the general possible complications of cataract surgery itself, which are distinct from the risks associated with inadequate lens selection preparation.
A contact lens simulation provides a real-world preview of how monofocal, multifocal, monovision, or extended depth-of-focus IOL corrections may feel during daily activities. Without that preview, patients lose a critical opportunity to evaluate visual trade-offs before committing to a permanent intraocular lens. According to findings presented at the 2024 ESCRS Meeting, a mismatch between expectations and outcomes can create a perceived loss of control among patients, which may foster regret, while effective preoperative simulation promotes a sense of agency and cognitive ownership.
Skipping the trial also weakens the foundation of informed consent. For consent to be valid, a patient must have received sufficient information to make a decision. A contact lens trial translates abstract IOL descriptions into lived experience, helping patients understand the potential limitations of options such as halos with multifocal lenses or depth perception changes with monovision.
From a clinical perspective, foregoing simulation is one of the more preventable oversights in the preoperative workflow. Patients who experience their correction before surgery tend to communicate more clearly with their surgeon about preferences, which can directly influence lens selection accuracy. The few days spent in a trial period represent a small investment compared to the permanence of an implanted lens.
Understanding these risks underscores why surgical education can further strengthen your preparation.
How Can Surgical Education Help You Prepare for Your Vision Decision?
Surgical education can help you prepare for your vision decision by translating complex lens options into clear, actionable knowledge. The sections below cover how Eye Surgery Today’s cataract guides clarify your choices and the key takeaways from simulating your vision plan with contact lenses.
Can Eye Surgery Today’s Cataract Surgery Guides Help You Understand Your Lens Options?
Yes, Eye Surgery Today’s cataract surgery guides can help you understand your lens options by breaking down the differences between monofocal, multifocal, EDOF, and monovision IOLs in clear, surgeon-authored language. Ophthalmologists continue to emphasize individualized decision-making when selecting intraocular lenses, starting with a thorough preoperative discussion of every available option.
Eye Surgery Today addresses the most common patient questions before cataract surgery, including:
- Which type of intraocular lens is best for me?
- Will I need glasses after surgery?
- What happens at my first cataract consultation?
According to Cataract & Refractive Surgery Today, visual simulators that offer a virtual preview of postoperative vision help patients understand potential benefits and limitations of various IOL options, assisting surgeons in optimizing outcomes and leading to more informed choices. Eye Surgery Today’s guides complement these simulation tools by providing the educational foundation patients need to interpret what they experience during a contact lens trial. When you understand each lens category before your appointment, the simulation becomes far more meaningful.
What Are the Key Takeaways About Simulating Your Vision Plan with Contact Lenses Before Surgery?
The key takeaways about simulating your vision plan with contact lenses before surgery center on informed preparation, realistic expectations, and active participation in your lens selection. Vision simulators encompass a range of tools, from digital IOL simulators and binocular wearable devices to real-world trials with contact lenses, each aiming to improve patients’ understanding of possible outcomes and strengthen their sense of agency.
Core lessons from the contact lens simulation process include:
- A real-world contact lens trial can reveal how monovision, multifocal, or EDOF correction feels during daily activities before any permanent surgical change.
- Simulation results should guide a collaborative conversation with your surgeon, not replace professional clinical assessment.
- Reliable education helps counter the widespread misinformation about contact lenses that, according to the American Optometric Association, could harm vision and eye health if left unaddressed.
No simulation perfectly replicates an implanted IOL, but combining hands-on lens trials with expert surgical education gives you the strongest foundation for a confident vision decision. Eye Surgery Today provides the resources to help you prepare for that conversation with clarity.
