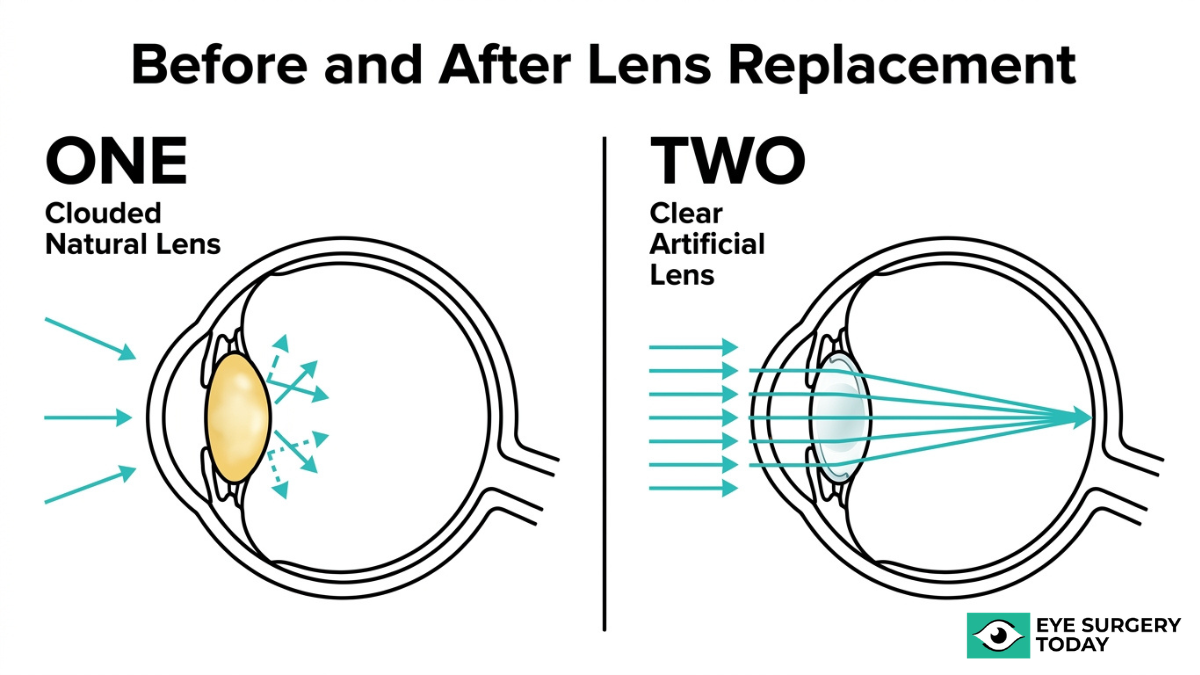
Light sensitivity after cataract surgery is a common visual response that occurs when the clouded natural lens is replaced with a clear artificial intraocular lens (IOL), allowing significantly more light to reach the retina than the eye has processed in years. Neuroadaptation is the brain’s parallel process of recalibrating how it interprets this new optical input over weeks to months.
This guide covers the physiological causes of post-surgical photophobia, how neuroadaptation works and its typical timeline, the different types of light sensitivity patients may experience, risk factors for prolonged symptoms, and practical management strategies during recovery.
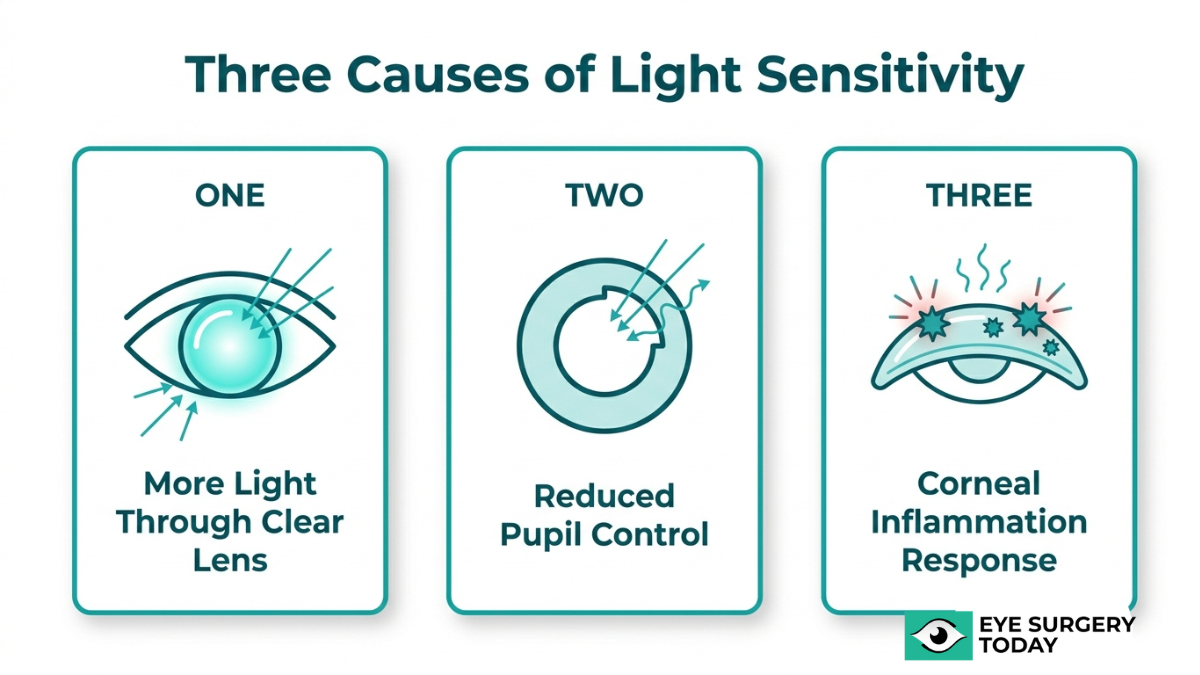
Removing the opaque crystalline lens increases light transmission while temporarily compromising pupil constriction, and corneal inflammation from surgical incisions can further scatter incoming light and lower the threshold for discomfort. Together, these mechanisms explain why brightness, glare, and halos often feel most intense in the early postoperative period.
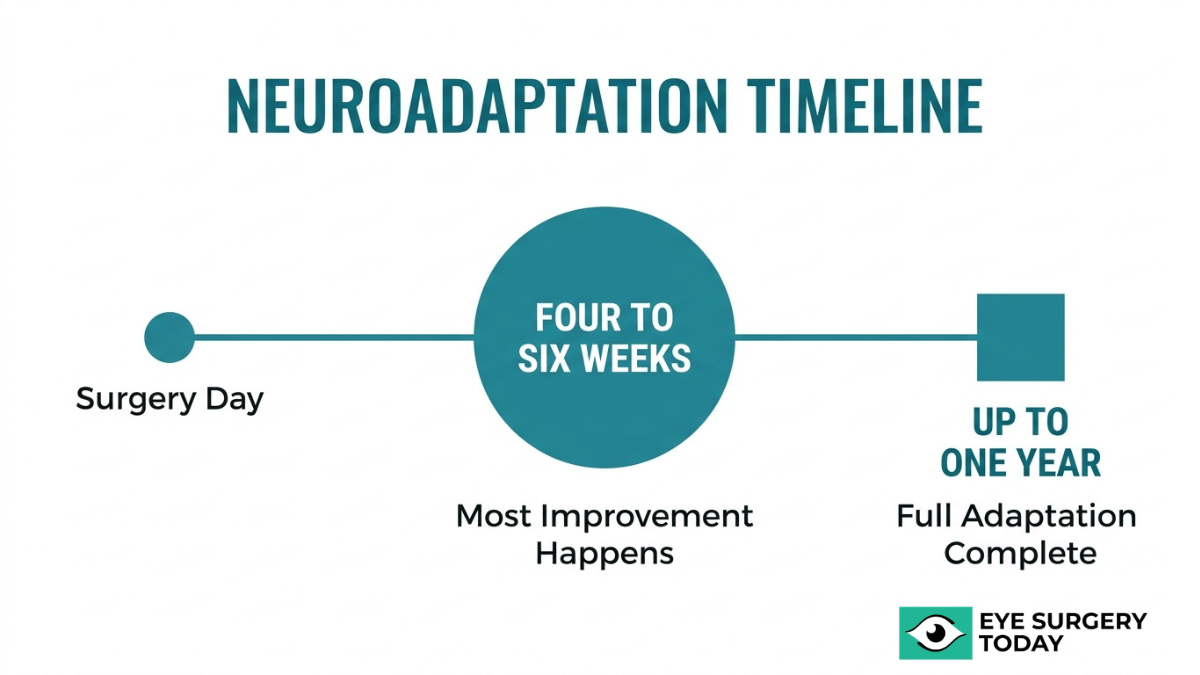
Neuroadaptation typically produces noticeable improvement by four to six weeks, though the full process can extend up to a year. During this period, the visual cortex progressively learns to suppress unwanted optical signals, such as edge reflections from the IOL, while prioritizing useful visual information.
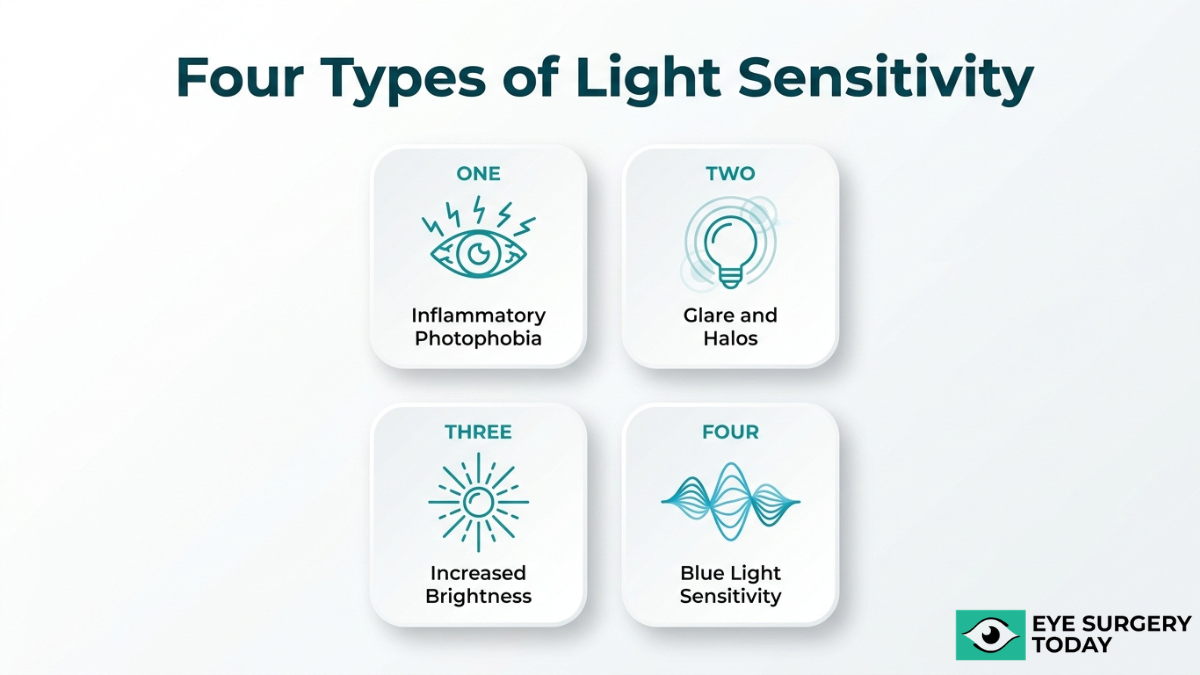
Post-surgical sensitivity can present as inflammatory photophobia, glare and halos from IOL optics, heightened brightness perception, or increased blue light exposure after removal of the eye’s natural UV filter. IOL type, pre-existing dry eye, and individual neural plasticity may all influence how long symptoms persist.
Persistent or worsening sensitivity that does not follow the expected recovery pattern may signal complications such as infection, chronic inflammation, or cystoid macular edema, and warrants prompt evaluation by an ophthalmologist.
Why Are Your Eyes More Sensitive to Light After Surgery?
Your eyes are more sensitive to light after surgery because removing the clouded natural lens dramatically increases light transmission, while temporary changes in pupil function and corneal inflammation amplify the effect.
How Does Removing the Natural Lens Change Light Entry?
Removing the natural lens changes light entry by replacing an opaque, yellowed crystalline lens with a clear artificial intraocular lens (IOL), which allows significantly more light to reach the retina. According to research published in Investigative Ophthalmology & Visual Science, the change in maximal pupil constriction following cataract surgery is consistent with an increase in light transmission into the eye after the opaque crystalline lens is removed.
This sudden flood of light can feel overwhelming because the eye has spent years adapting to reduced input. The clear IOL also introduces a new optical edge that was absent with the natural lens. As light strikes this edge, it can scatter in ways the brain does not yet recognize. These scattered rays may appear as streaks, arcs, or flickers in the peripheral vision, a phenomenon known as positive dysphotopsia. For most patients, the intensity of this brightness perception gradually decreases as the visual system recalibrates.
What Role Does Pupil Dilation Play in Post-Surgical Glare?
Pupil dilation plays a significant role in post-surgical glare because the pupil’s ability to constrict and regulate incoming light can be temporarily compromised after cataract surgery. A study published in the National Library of Medicine (PubMed) found that the mean percentage of pupillary constriction was significantly reduced at one and three months postoperatively compared with preoperative levels (P<.0001), suggesting that cataract surgery may compromise pupillary constriction and dilation functions.
When the pupil cannot constrict efficiently, more light enters the eye than the retina needs, especially in bright environments. This reduced regulation makes glare, halos, and starbursts more noticeable around light sources. Age-related factors can further slow the pupil’s recovery, extending the period of heightened sensitivity. In most cases, pupillary function gradually improves as healing progresses, though the timeline varies from patient to patient.
How Does Corneal Inflammation Contribute to Sensitivity?
Corneal inflammation contributes to sensitivity by disrupting the smooth optical surface of the cornea, causing incoming light to scatter rather than focus cleanly on the retina. During cataract surgery, small incisions in the cornea trigger a natural inflammatory response. Even mild postoperative swelling, known as corneal edema, can diffuse light and intensify the perception of brightness, glare, and discomfort.
This inflammation also affects the corneal nerve endings, which are among the most densely innervated tissues in the body. Irritated nerves lower the threshold for light-induced discomfort, making even moderate illumination feel painful. Conditions such as persistent iritis or pre-existing dry eye can prolong this inflammatory cycle. Anti-inflammatory eye drops prescribed during recovery directly target this mechanism, and in clinical practice, addressing corneal inflammation early is one of the most effective ways to accelerate visual comfort after surgery.
With these physiological factors understood, the brain’s own adaptation process plays an equally important role in resolving post-surgical light sensitivity.
What Is Neuroadaptation After Cataract Surgery?
Neuroadaptation after cataract surgery is the brain’s process of adjusting to visual input from a new intraocular lens. The following sections explain how this adjustment works, its typical timeline, and the visual changes patients may notice during recovery.
How Does the Brain Adjust to a New Intraocular Lens?
The brain adjusts to a new intraocular lens by gradually recalibrating how it processes unfamiliar visual signals. When a clouded natural lens is replaced with an artificial IOL, the visual cortex receives sharper, brighter input than it has processed in months or years. Initially, this mismatch can produce perceptual disturbances, including heightened glare sensitivity, mild halos, or shifts in color perception.
Over time, neural pathways adapt to interpret the new optical data as normal. According to the American Academy of Ophthalmology, neuroadaptation is a process in which the brain reacts to a new intraocular lens, with most patients experiencing symptom improvement at around four to six weeks postoperatively, though it can take up to a year in some cases.
Patience during this period is essential. The brain is remarkably capable of recalibrating its visual processing, but the adjustment is not instantaneous. Patients often seek clear insights into their before and after vision results and what expected improvements they can anticipate.
How Long Does Neuroadaptation Typically Take?
Neuroadaptation typically takes four to six weeks for most patients, though the full recovery process can extend up to 12 months depending on several factors. Key variables that influence this timeline include:
- IOL type: Multifocal and extended depth-of-focus lenses often require longer adaptation than monofocal designs because the brain must learn to select between multiple focal points.
- Pre-surgical visual state: Patients with dense cataracts may experience a more dramatic change in light transmission, which can extend the adjustment period.
- Individual neural plasticity: Age and overall neurological health can affect how quickly visual processing pathways recalibrate.
Most noticeable improvement occurs within the first six weeks. If symptoms persist beyond several months without gradual improvement, a follow-up evaluation with a surgeon may be appropriate to rule out other contributing factors.
What Visual Changes Occur During Neuroadaptation?
The visual changes that occur during neuroadaptation can include increased brightness perception, mild halos or starbursts around light sources, slight color shifts, and temporary difficulty adjusting between different lighting environments. These phenomena reflect the brain’s incomplete processing of input from the new IOL, not a problem with the lens itself.
Color perception shifts, particularly a subtle blue tint known as cyanopsia, are common in the early postoperative period as the brain adjusts to increased short-wavelength light reaching the retina. Glare and starburst effects tend to be most pronounced at night or in high-contrast lighting conditions.
For most patients, these visual disturbances diminish progressively as neuroadaptation advances. Understanding that these changes are a normal part of recovery, rather than a sign of surgical complications, can help reduce unnecessary concern during the healing process.
What Types of Light Sensitivity Can Occur After Surgery?
The types of light sensitivity that can occur after cataract surgery include photophobia from inflammation, glare and halos, increased brightness perception, and blue light sensitivity.
Photophobia From Surgical Inflammation
Photophobia from surgical inflammation is a direct light intolerance triggered by postoperative irritation inside the eye. When cataract surgery disturbs intraocular tissues, the resulting inflammatory response can sensitize the iris and ciliary body, making even moderate light uncomfortable. This type of sensitivity typically feels like a diffuse, aching discomfort rather than a specific visual distortion. Because inflammation is the underlying driver, photophobia from this cause tends to respond well to prescribed anti-inflammatory treatment during recovery. Of all the post-surgical light sensitivity types, this one is often the most straightforward to identify and manage with your surgeon’s guidance.
Glare and Halos Around Lights
Glare and halos around lights are optical disturbances caused by the way light interacts with the edge or surface of an artificial intraocular lens. Patients often notice bright rings surrounding headlights or streetlamps, particularly at night. According to Dr. Gregory W. Bligard, MD, PhD, and Dr. Linda M. Tsai, MD, “multifocal and extended depth-of-focus IOLs may also cause optical disturbances such as halos, glare, or starbursts around light sources, particularly at nighttime.” These phenomena, classified as positive dysphotopsias, differ from photophobia because they involve specific visual artifacts rather than generalized discomfort. For many patients, nighttime driving presents the most noticeable challenge during early recovery.
Increased Brightness Perception From Clearer Optics
Increased brightness perception from clearer optics occurs because the new intraocular lens transmits significantly more light than the clouded natural lens it replaced. A cataract acts as a built-in filter, gradually dimming and yellowing incoming light over years. Once removed, colors may appear more vivid and indoor lighting can feel unexpectedly intense. This heightened perception is not a complication; it reflects the eye receiving a more accurate volume of light. Most patients find this initial brightness overwhelming but ultimately beneficial, as the brain recalibrates its expectations through neuroadaptation over several weeks.
Blue Light Sensitivity After UV-Filtering Lens Removal
Blue light sensitivity after UV-filtering lens removal results from the sudden increase in short-wavelength light reaching the retina. The aging natural lens progressively absorbs blue light below 500 nm, so its removal allows wavelengths the eye had not processed in years to pass through freely. Some intraocular lenses include blue-light filtering properties to reduce this effect. A Cochrane Library review found that distance best-corrected visual acuity with a blue-light filtering IOL at six to 18 months postoperatively was not clearly different from that with a non-blue-light filtering IOL (mean difference -0.01 logMAR, 95% CI -0.03 to 0.02), suggesting lens filter choice does not compromise visual outcomes.
Understanding each sensitivity type helps clarify which symptoms warrant routine patience and which may need clinical attention.
How Does Neuroadaptation Help Reduce Light Sensitivity?
Neuroadaptation helps reduce light sensitivity by retraining the brain’s visual processing centers to suppress unwanted optical signals from a new intraocular lens. The following subsections explain how glare filtering develops, whether halos fully resolve, and what may happen when adaptation stalls.
How Does the Brain Learn to Filter Unwanted Glare?
The brain learns to filter unwanted glare through a gradual recalibration of visual cortex activity in response to changed light input after cataract surgery. When an artificial intraocular lens replaces the natural crystalline lens, the brain initially registers unfamiliar light patterns, including edge reflections and increased brightness, as distracting visual noise. Over weeks and months, neural circuits begin selectively suppressing these signals while prioritizing useful visual information.
According to a 2021 study published in Frontiers in Neuroscience, early postoperative visual neuroadaptation was detected in multifocal IOL patients by resting-state fMRI analysis, with visual cortex fALFF values decreasing at one week postoperatively, recovering to baseline at three months, and improving beyond preoperative levels at six months. This progressive cortical reorganization reflects the brain actively learning which light signals to amplify and which to dampen. For most patients, this filtering process unfolds without conscious effort, though individual timelines vary depending on IOL type and baseline neural plasticity.
Can Neuroadaptation Fully Resolve Halos and Starbursts?
Neuroadaptation can significantly reduce halos and starbursts for most patients, though complete resolution is not guaranteed in every case. These photic phenomena occur because the IOL edge refracts light differently than the natural lens, producing peripheral bright artifacts. As the visual cortex adapts, the brain progressively downregulates its response to these optical disturbances, making them less noticeable over time.
According to the American Academy of Ophthalmology, most patients experience improvement of dysphotopsia symptoms at around four to six weeks postoperatively, though full adaptation can take up to a year in some cases. Multifocal and extended depth-of-focus IOLs may produce more persistent optical disturbances than monofocal designs, because they split light into multiple focal points. Even when halos do not vanish entirely, many patients report that the symptoms become manageable enough to no longer interfere with daily activities. The degree of final resolution depends on the interplay between IOL optics, pupil dynamics, and each individual’s neuroadaptive capacity.
What Happens When Neuroadaptation Stalls or Is Incomplete?
When neuroadaptation stalls or is incomplete, patients may continue experiencing bothersome glare, halos, or general light sensitivity well beyond the typical recovery window. Several factors can contribute to this plateau:
- Underlying ocular surface conditions, such as dry eye or blepharitis, can perpetuate photophobia and interfere with clear image formation on the retina.
- Persistent low-grade inflammation, including subclinical iritis, may sustain light sensitivity independently of neuroadaptive progress.
- Psychological factors can play a role; as Dr. Gary S. Hirshfield, MD, notes through the AAO, some patients develop anxiety about postoperative brightness changes that may cause a persistent disturbance.
- IOL-related optical properties, particularly with multifocal designs, may produce photic phenomena that exceed the brain’s capacity to fully suppress.
When symptoms persist beyond six to twelve months, an ophthalmologist should evaluate for treatable causes before attributing the issue solely to incomplete neuroadaptation. In rare cases, IOL exchange may be considered if optical disturbances remain functionally limiting.
With an understanding of when neuroadaptation may fall short, identifying which patients face higher risk becomes the next consideration.
Who Is More Likely to Experience Prolonged Sensitivity?
Prolonged light sensitivity after cataract surgery can depend on IOL type, optical design complexity, and pre-existing ocular surface conditions. The following subsections cover how each factor may influence recovery duration.
Does IOL Type Affect How Long Light Sensitivity Lasts?
IOL type can affect how long light sensitivity lasts. Monofocal lenses produce a single focal point, which typically generates fewer unwanted optical phenomena during recovery. Multifocal and extended depth-of-focus IOLs split incoming light across multiple focal zones, a design that may increase the brain’s neuroadaptation workload. Because these advanced lenses demand more complex visual processing, patients who receive them sometimes report glare, halos, or starbursts for a longer period before symptoms gradually diminish. The optical profile of the chosen IOL is one of the most underappreciated factors in setting realistic recovery expectations before surgery, including preparing for possible glasses use.
Are Patients With Multifocal IOLs More Prone to Glare?
Patients with multifocal IOLs are generally more prone to glare than those with monofocal lenses. The concentric ring design that enables near and distance vision simultaneously can scatter light at ring edges, producing halos and starbursts, especially under low-light conditions. According to a 2021 resting-state fMRI study published in Frontiers in Neuroscience, early postoperative visual neuroadaptation was detected in multifocal IOL patients, with visual cortex activity decreasing at one week, recovering to baseline at three months, and improving beyond preoperative levels at six months. This timeline suggests the brain actively recalibrates its processing of multifocal optics over several months, and glare symptoms often follow a parallel course of gradual resolution.
Does Pre-Existing Dry Eye Worsen Post-Surgical Sensitivity?
Pre-existing dry eye can worsen post-surgical light sensitivity. An irregular or unstable tear film scatters incoming light across the corneal surface, amplifying glare and photophobia that would otherwise remain mild. Cataract surgery itself may temporarily reduce tear production due to corneal nerve disruption during the incision, compounding sensitivity in patients whose ocular surface was already compromised. Managing dry eye before and after surgery, through preservative-free artificial tears or other treatments your eye doctor may recommend, can help reduce the severity and duration of postoperative discomfort.
Understanding individual risk factors helps set appropriate expectations for the recovery timeline ahead.
What Are the Possible Risks If Sensitivity Does Not Improve?
The possible risks if sensitivity does not improve include underlying complications such as infection, chronic inflammation, or cystoid macular edema. The sections below cover when persistent photophobia may signal a problem and which conditions your surgeon should rule out.
When Could Persistent Light Sensitivity Signal a Complication?
Persistent light sensitivity could signal a complication when it does not follow the expected recovery timeline or worsens after initial improvement. According to the American Academy of Ophthalmology, extreme light sensitivity can be a sign of infection after cataract surgery, and patients experiencing this should call their ophthalmologist right away. Increasing pain, redness, or sudden visual changes alongside photophobia may also indicate:
- Endophthalmitis (intraocular infection)
- Chronic or recurrent iritis
- Cystoid macular edema
- IOL malposition causing persistent dysphotopsia
Sensitivity that remains severe beyond six to eight weeks, rather than gradually fading, warrants prompt evaluation. In clinical practice, delayed presentation of these complications often leads to more difficult management, making early recognition one of the most important factors in preserving visual outcomes.
What Conditions Should Be Ruled Out by Your Surgeon?
The conditions that should be ruled out by your surgeon include persistent iritis, cystoid macular edema, elevated intraocular pressure, IOL dislocation, and retained lens fragments. Each of these can produce ongoing photophobia that mimics normal postoperative sensitivity but requires targeted treatment.
Your ophthalmologist may perform a slit-lamp examination, optical coherence tomography, or intraocular pressure measurement to differentiate between benign adaptation and a treatable condition. Ocular surface disorders, particularly dry eye disease and blepharitis, should also be excluded because they frequently contribute to prolonged discomfort after surgery. When these conditions are identified early, anti-inflammatory therapy or surgical intervention can often restore comfort and visual quality.
Understanding which complications require attention helps frame realistic expectations for managing light sensitivity during recovery.
What Can Help Manage Light Sensitivity During Recovery?
Several strategies can help manage light sensitivity during recovery, including protective eyewear, prescribed anti-inflammatory drops, and careful light exposure habits.
Do Photochromic or Tinted Lenses Help After Surgery?
Photochromic or tinted lenses can help reduce discomfort from bright light after cataract surgery. Photochromic lenses automatically darken in response to UV exposure, limiting the amount of light reaching the retina during outdoor activities. Tinted lenses with amber or gray shading may also reduce glare perception in high-contrast environments.
These options work best as temporary comfort measures during the early postoperative weeks, when the eye is still adjusting to increased light transmission through the new intraocular lens. Wraparound styles offer additional protection by blocking peripheral light. However, relying on very dark lenses indoors for extended periods is generally discouraged, as it may delay the eye’s natural adjustment to normal lighting conditions. Your ophthalmologist can recommend the appropriate tint level based on your specific symptoms and IOL type.
Can Anti-Inflammatory Eye Drops Speed Up Comfort?
Anti-inflammatory eye drops can help speed up comfort by treating one of the most common treatable causes of post-surgical photophobia: persistent iritis. According to the American Academy of Ophthalmology, the main treatable causes for photophobia after cataract surgery include persistent iritis, significant dry eyes, and surface conditions such as blepharitis, all of which may respond to anti-inflammatory therapy.
Ophthalmologists typically prescribe a combination of topical corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs) during the early recovery period. By controlling inflammation at the surgical site, these drops can reduce the irritation that amplifies light sensitivity. Following the prescribed drop schedule consistently is important; skipping doses may allow inflammation to rebound, prolonging discomfort. If photophobia persists despite consistent drop use, your surgeon may need to evaluate for underlying complications.
Does Gradual Light Exposure Support Neuroadaptation?
Gradual light exposure may support neuroadaptation, though specific light exposure protocols lack strong evidence from large randomized controlled trials. The concept is based on the principle that controlled, incremental increases in ambient brightness could help the brain recalibrate its visual processing after receiving a new IOL.
In practice, many clinicians suggest starting with dimmer indoor environments immediately after surgery and slowly introducing brighter settings over several weeks. This approach aligns with general neuroadaptation principles, where the visual cortex progressively adjusts to new optical input. Still, no standardized protocol has been validated, so any gradual exposure plan should be guided by individual comfort rather than a rigid schedule. Patience remains essential; the brain’s adjustment timeline varies significantly between patients.
With management strategies in place, understanding the broader context of post-surgical vision changes helps set realistic expectations.
How Should You Approach Post-Surgical Vision Changes?
You should approach post-surgical vision changes by relying on surgeon-reviewed guidance and understanding the key principles of recovery. The sections below cover how expert resources can support your recovery and the most important takeaways about light sensitivity and neuroadaptation.
Can Surgeon-Reviewed Cataract Surgery Guidance Help You?
Yes, surgeon-reviewed cataract surgery guidance can help you distinguish normal recovery patterns from symptoms that may require medical attention. After cataract surgery, many patients experience some degree of light sensitivity, glare, or visual disturbances that resolve naturally as neuroadaptation progresses. However, not all symptoms are benign. According to Cataract & Refractive Surgery Today, chronic or recurrent inflammation, including cystoid macular edema, occurs in approximately 0.1% to 2% of patients following routine cataract surgery.
Surgeon-reviewed resources provide clarity on several critical recovery topics:
- Recognizing treatable causes of photophobia, such as persistent iritis, dry eyes, and blepharitis
- Understanding when light sensitivity warrants an urgent call to your ophthalmologist
- Learning which visual phenomena, such as halos or starbursts, typically improve with time
- Knowing what anti-inflammatory treatment options your surgeon may recommend
Platforms like Eye Surgery Today offer content reviewed by practicing surgeons, helping patients navigate these questions with confidence rather than uncertainty.
What Are the Key Takeaways About Light Sensitivity and Neuroadaptation?
The key takeaways about light sensitivity and neuroadaptation center on three principles: most post-surgical sensitivity is temporary, the brain actively adapts to new visual input, and persistent symptoms deserve prompt evaluation.
Light sensitivity after cataract surgery results from increased light transmission through a clear intraocular lens replacing the opaque natural lens. The brain needs time to recalibrate its response to this brighter input. Neuroadaptation typically begins within the first week and often produces noticeable improvement by four to six weeks, though complete adjustment can take up to a year for some individuals.
The most actionable conclusions from this article include:
- Photophobia, glare, and halos are common early symptoms that frequently resolve without intervention.
- Multifocal and extended depth-of-focus IOLs may cause more pronounced optical disturbances initially.
- Anti-inflammatory drops can address treatable causes of prolonged sensitivity.
- Extreme or worsening light sensitivity may signal infection or chronic inflammation and requires immediate evaluation.
- Gradual light exposure may support comfort during recovery, though structured protocols lack strong clinical trial evidence.
Informed patients recover with less anxiety. Eye Surgery Today provides surgeon-reviewed educational resources designed to help you understand every stage of your cataract surgery journey, from pre-operative preparation through full visual recovery.
