Dry eye is a chronic ocular surface condition that can compromise the accuracy of intraocular lens calculations and the quality of vision recovery after cataract surgery. An unstable tear film distorts the corneal measurements surgeons use to select lens power, and the surgical procedure itself may worsen dryness during the healing period.
This guide covers how dry eye disrupts preoperative measurements, how different dry eye subtypes affect surgical planning, diagnostic and treatment protocols before lens calculations, surgical factors that may worsen dryness during recovery, and risk factors alongside long-term management strategies.
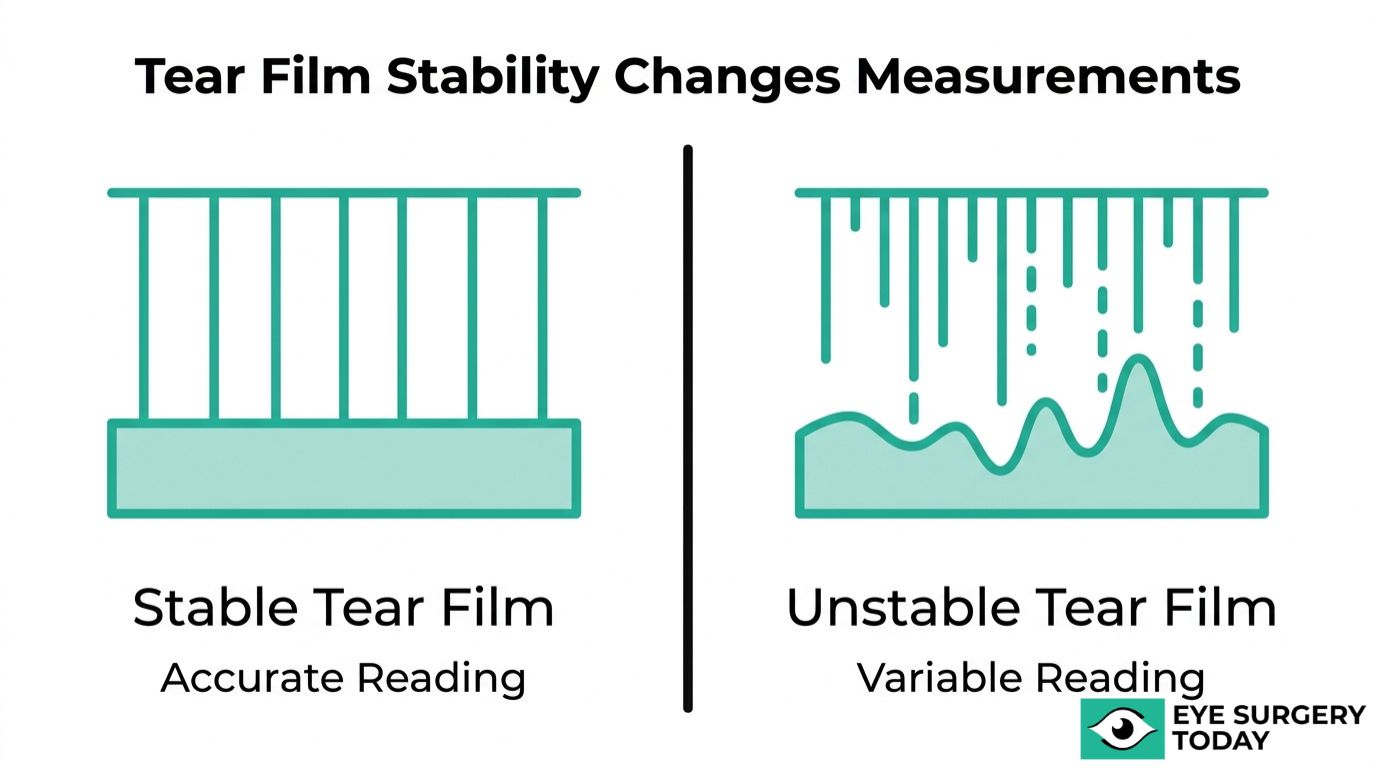
Tear film instability can shift keratometry readings, potentially leading to an IOL power selection that misses the intended refractive target. Corneal topography is similarly affected, as an irregular tear film can distort the corneal surface and produce unreliable maps, while optical biometry is less impacted overall, with axial length measurements remaining relatively stable.
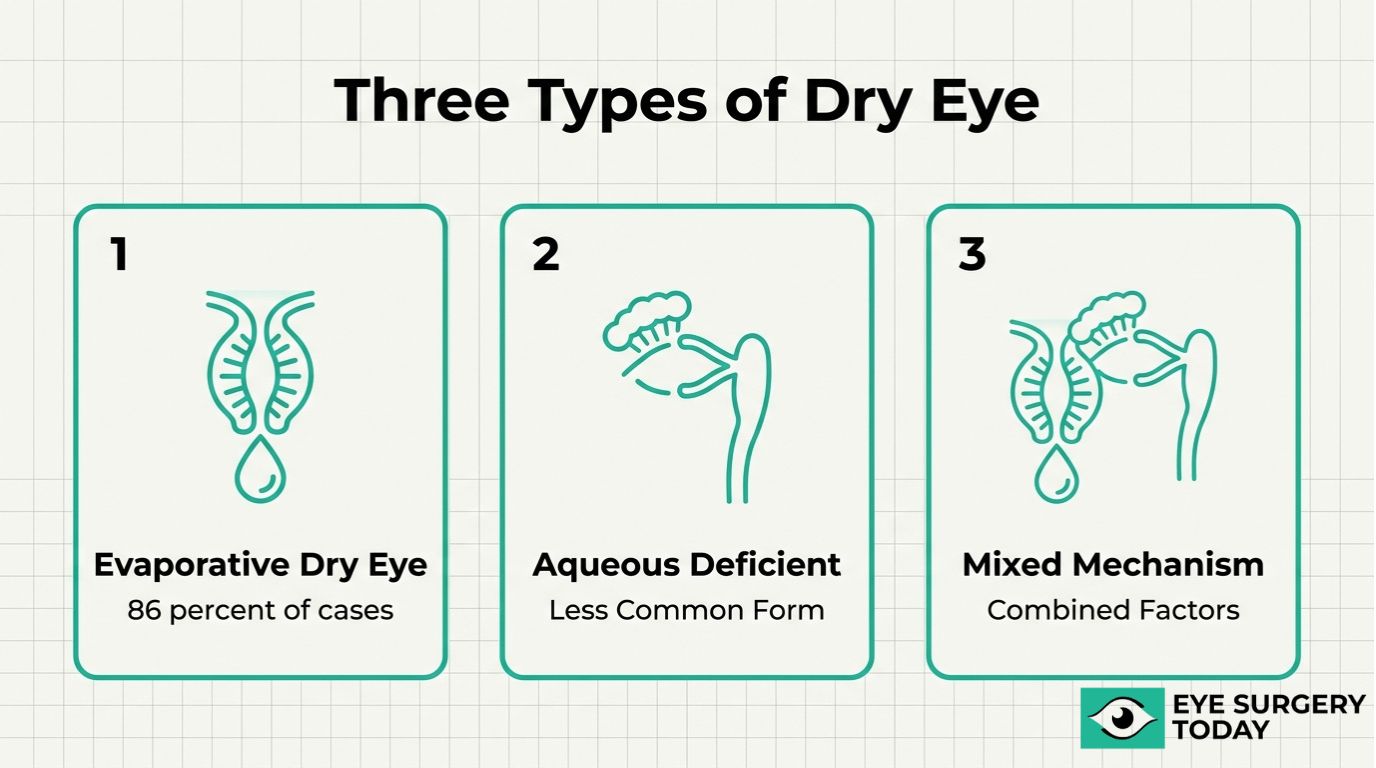
Evaporative, aqueous-deficient, and mixed-mechanism dry eye each present distinct measurement challenges. Evaporative dry eye caused by meibomian gland dysfunction is the most common form and is often linked to tear film instability that can produce irregular or inconsistent astigmatism measurements as well as compromise toric and premium IOL planning.
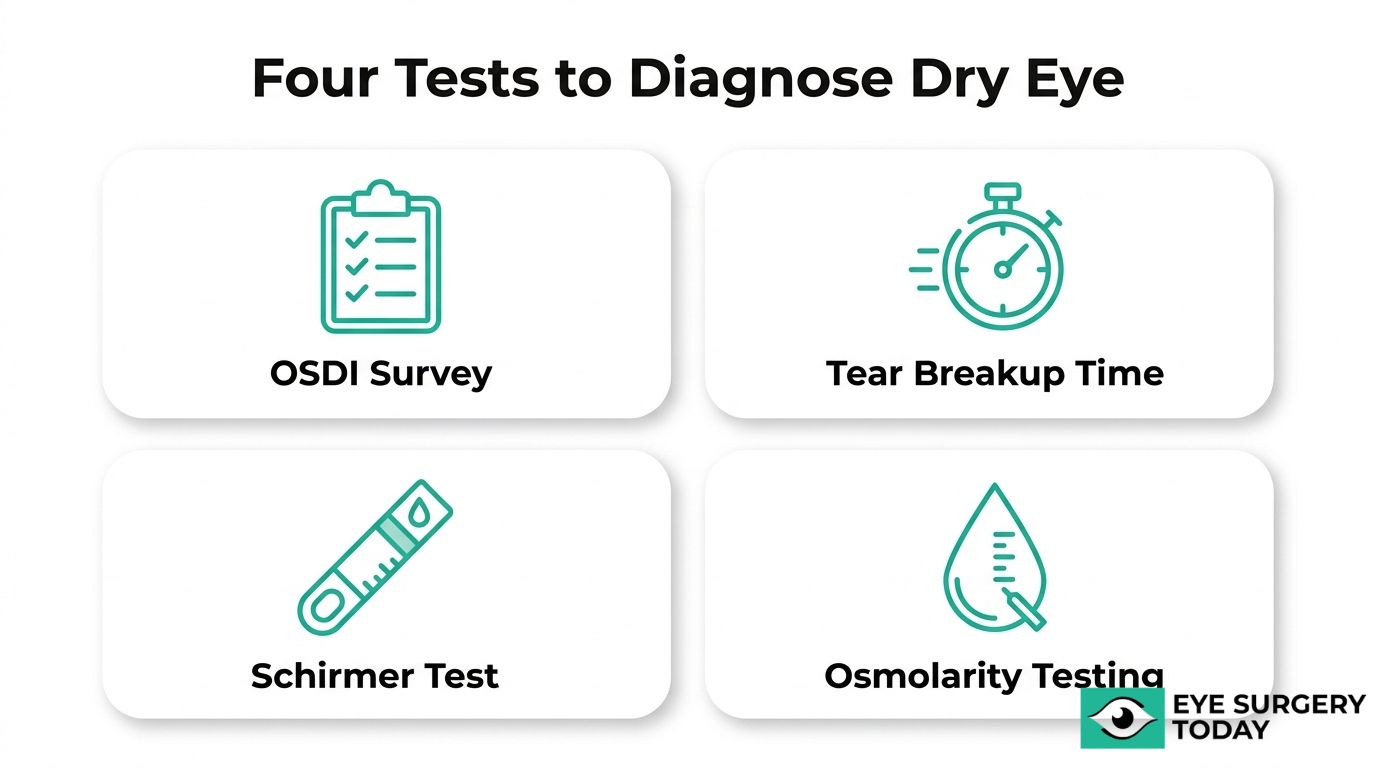
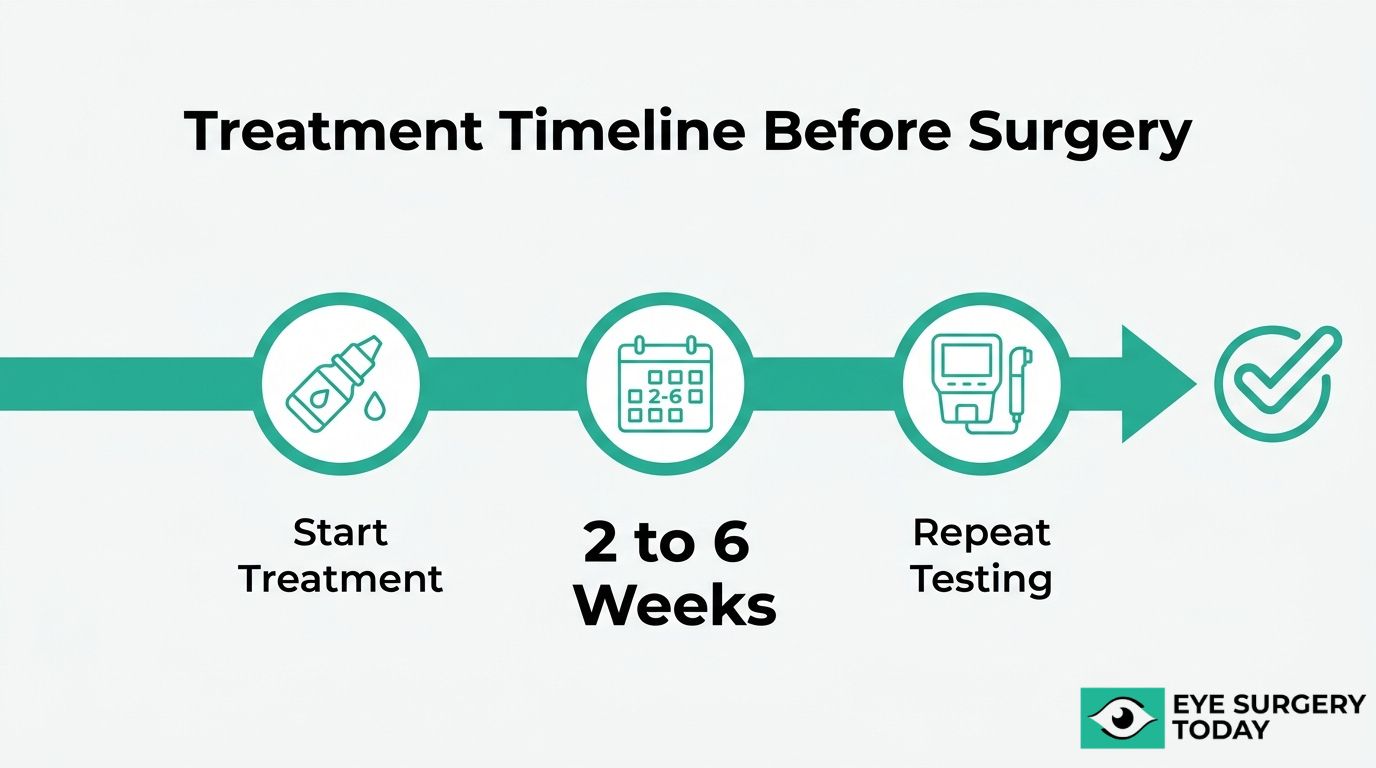
Validated screening tools, including symptom questionnaires, tear breakup time, and osmolarity testing, can identify disease that patients themselves may not notice. A stepwise treatment approach using preservative-free lubricants, anti-inflammatory drops, or in-office gland therapies may help stabilize the ocular surface before repeat biometry is performed.
Cataract surgery can worsen dry eye through corneal nerve disruption, microscope light exposure, and preservative-containing postoperative drops. Symptoms typically peak within the first week and may persist for several months, though structured recovery protocols can resolve discomfort in the majority of patients over time.
Older adults, patients with autoimmune conditions, and long-term contact lens wearers face elevated risk. Recognizing these factors early and managing dry eye before finalizing surgical plans is one of the most effective steps toward accurate lens selection and a satisfying visual outcome.
What Is Dry Eye and Why Does It Matter Before Cataract Surgery?
Dry eye is a chronic ocular surface condition that can compromise the accuracy of cataract surgery planning and the quality of postoperative vision. The following sections explain how the tear film functions and why dry eye is so prevalent among cataract candidates.
How Does the Tear Film Influence the Surface of the Eye?
The tear film influences the surface of the eye by maintaining a smooth, stable optical layer that light must pass through before reaching internal structures. According to the Tear Film & Ocular Surface Society (TFOS) DEWS II definition, dry eye is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, accompanied by ocular symptoms in which tear film instability, hyperosmolarity, ocular surface inflammation, and neurosensory abnormalities play etiological roles.
When this protective layer breaks down, the corneal surface becomes irregular. That irregularity distorts the measurements surgeons rely on to select the correct intraocular lens. Surgical conditions can further destabilize the tear film, as exposure to intense operating microscope light has been shown to induce phototoxic damage to the ocular surface, including inflammation and reduced goblet cell density.
For patients approaching cataract surgery, even mild tear film disruption that goes unnoticed in daily life can meaningfully alter preoperative data quality.
Why Is Dry Eye So Common in Cataract Surgery Candidates?
Dry eye is so common in cataract surgery candidates because this population shares overlapping risk factors, including advanced age, chronic medication use, and prolonged screen exposure. The landmark PHACO study published in the Journal of Cataract & Refractive Surgery (Trattler et al., 2017) revealed that 77% of eyes evaluated for cataract surgery had corneal staining, and 62.9% had a tear breakup time (TBUT) of 5 seconds or less.
These numbers suggest that the majority of cataract patients already have a compromised ocular surface before surgery even begins. What makes this especially consequential is that a 1.0 diopter error in corneal power measurement translates to approximately a 1.0 diopter error in the predicted refractive outcome. In practice, this means a surgeon could select the wrong lens power simply because the tear film was unstable during testing.
Many of these patients remain undiagnosed because they attribute dryness symptoms to normal aging. Proactive screening before cataract surgery is one of the most effective steps toward accurate lens selection and a satisfying visual result.
How Does Dry Eye Distort Intraocular Lens Calculations?
Dry eye distorts intraocular lens calculations by creating an irregular optical surface that compromises the accuracy of keratometry, corneal topography, and optical biometry. The following subsections explain each measurement error.
How Does an Unstable Tear Film Affect Keratometry Readings?
An unstable tear film affects keratometry readings by introducing measurement variability that can significantly alter the calculated intraocular lens power. Keratometry depends on light reflecting off a smooth, uniform tear layer to determine corneal curvature. When that layer breaks up unevenly, the reflected signal fluctuates, producing inconsistent readings between consecutive measurements.
A 2024 study in Scientific Reports (Ahn et al.) demonstrated that dry eye–related tear film instability increases variability in keratometry measurements, which can lead to clinically significant differences in intraocular lens (IOL) power calculations and a higher risk of postoperative refractive error. Variability in corneal power measurements can translate into meaningful refractive differences, as approximately 1.0 diopter at the corneal plane corresponds to about 0.7–0.8 diopters at the spectacle plane. For patients expecting clear vision without glasses after surgery, even half a diopter of unexpected error may feel like a disappointing outcome. Stabilizing the tear film before obtaining keratometry readings remains one of the most important steps in the preoperative workflow.
How Does Dry Eye Cause Errors in Corneal Topography?
Dry eye causes errors in corneal topography by disrupting the smooth reflective surface that topographic instruments rely on to map corneal curvature. Placido disc systems, the most widely used topography technology, project concentric rings of light onto the tear film. When dry patches or debris scatter that light, the resulting map displays artificially irregular astigmatism patterns that do not reflect the true corneal shape.
These false readings are particularly problematic for toric IOL planning, where even minor axis misalignment can reduce the intended astigmatism correction. Compounding the issue, preservatives in some perioperative eye drops may worsen surface irregularity. According to a 2024 report in Clinical Ophthalmology (Jensen et al.), benzalkonium chloride (BAK) in postoperative drops can cause significant toxic effects on the corneal epithelium and aggravate dry eye symptoms during early recovery. There is growing clinical preference for preservative-free formulations to protect topographic accuracy at follow-up visits.
How Does Tear Film Irregularity Alter Optical Biometry Results?
Tear film irregularity alters optical biometry results because reflected light signals that optical biometers rely on become distorted and thus affect the results from the instruments used to measure axial length and corneal power simultaneously. Devices such as the IOLMaster and Lenstar pass coherent light through the tear film; an uneven surface scatters that beam, increasing signal noise and reducing measurement accuracy.
When the instrument’s software receives poor-quality scans, it may average unreliable data points or require multiple capture attempts, each yielding slightly different values. This variability feeds directly into IOL power formulas, where small input errors propagate into clinically meaningful refractive misses. In practice, repeated biometry sessions that produce inconsistent readings are often the first clinical clue that an unstable ocular surface needs treatment before surgical planning proceeds.
How Can Dry Eye Lead to Incorrect IOL Power Selection?
Dry eye can lead to incorrect IOL power selection because every formula used to choose a lens depends on accurate corneal and biometric inputs. When keratometry, topography, and biometry are each individually compromised by tear film instability, the cumulative error compounds through the calculation.
Modern formulas such as Barrett Universal II and Kane weight corneal power heavily. If the measured K-values are steeper or flatter than reality by even 0.5 D, the formula recommends a lens power that targets the wrong focal point. For premium lenses, including multifocal and extended depth of focus designs, the tolerance for error is especially narrow because these optics split light into multiple focal zones. Mismatched power in a premium IOL does not simply blur vision; it can create disabling glare, halos, or reduced contrast that may ultimately require lens exchange. Addressing dry eye before finalizing any lens selection is the most reliable way to prevent these avoidable outcomes.
What Types of Dry Eye Have the Greatest Impact on Preoperative Measurements?
Types of dry eye with impact on preoperative measurements include evaporative, aqueous-deficient, and mixed-mechanism dry eye. Each subtype disrupts the tear film differently, creating distinct challenges for accurate biometry.
Evaporative Dry Eye From Meibomian Gland Dysfunction
Evaporative dry eye from meibomian gland dysfunction (MGD) is the most prevalent and disruptive subtype for preoperative lens calculations. MGD causes the meibomian glands to produce insufficient or poor-quality lipid secretions, leading to rapid tear film evaporation. This instability creates an irregular corneal surface that distorts keratometry and topography readings.
According to a 2012 study published in Cornea (Lemp et al.), evaporative dry eye affects approximately 50% of patients with dry eye disease, while an additional 36% have a mixed etiology. Together, these evaporative-related forms account for roughly 86% of cases, making them the dominant subtype encountered during cataract evaluations. Because EDE is more frequently associated with irregular astigmatism on corneal topography, it can directly compromise toric IOL alignment calculations. For surgeons planning premium lens implantation, identifying and treating MGD before taking measurements is one of the most impactful steps in the entire preoperative workflow.
Aqueous-Deficient Dry Eye
Aqueous-deficient dry eye (ADDE) results from reduced tear production by the lacrimal glands. Conditions such as Sjögren’s syndrome, age-related lacrimal gland atrophy, and certain medications can diminish the aqueous layer of the tear film. With less fluid volume on the corneal surface, optical biometry devices may capture inconsistent axial length and keratometry values.
Although ADDE is less common than evaporative dry eye, its effect on measurement reproducibility should not be underestimated. A thinner aqueous layer accelerates tear breakup, and patients often show low Schirmer test scores alongside fluctuating refraction readings. Stabilizing tear volume through appropriate therapy before biometry helps ensure that the data guiding IOL power selection reflects the cornea’s true shape rather than a transiently dry surface.
Mixed-Mechanism Dry Eye
Mixed-mechanism dry eye involves both aqueous deficiency and increased evaporation occurring simultaneously, accounting for roughly 36% of cases. This combination compounds tear film instability, making preoperative measurements particularly unreliable without targeted treatment of each contributing factor.
According to the ASCRS Cornea Clinical Committee (Starr et al., 2019), mixed-mechanism dry eye represents a significant portion of the cataract population and requires comprehensive ocular surface optimization to ensure biometric reproducibility. Because two disruption pathways are active at once, standard single-therapy approaches may fall short. Clinicians often need to address both lipid layer quality and aqueous volume before repeating biometry. In clinical practice, mixed-mechanism dry eye can contribute to significant measurement variability, as it combines both reduced tear volume and tear film instability, which are key factors affecting keratometry and corneal topography. This makes thorough preoperative screening essential for accurate IOL selection.
With each dry eye subtype presenting distinct challenges, targeted diagnostic testing can help identify which mechanism is at play before surgery planning begins.
How Should Dry Eye Be Diagnosed Before Cataract Surgery?
Dry eye should be diagnosed before cataract surgery using a combination of validated questionnaires, clinical tests, and objective measurements. The following subsections cover specific diagnostic tests and why asymptomatic disease requires screening.
What Diagnostic Tests Help Identify Dry Eye Preoperatively?
The diagnostic tests that help identify dry eye preoperatively include symptom questionnaires, tear stability assessments, tear production measurements, and osmolarity testing. The Ocular Surface Disease Index (OSDI) questionnaire screens for subjective symptoms, while tear breakup time (TBUT) evaluates tear film stability on the corneal surface. The Schirmer test measures aqueous tear production, and tear osmolarity testing quantifies the salt concentration of the tear film.
According to a 2014 study published in PLOS ONE (Alves et al.), combining the OSDI, TBUT, and Schirmer test achieved a reported sensitivity of 100% and specificity of 95% for diagnosing dry eye disease. No single test captures every subtype, so a multi-test protocol gives the most reliable picture of ocular surface health before biometry readings are taken. In clinical practice, this layered approach is one of the most effective ways to catch disease that would otherwise compromise lens power calculations.
Can Dry Eye Be Present Without Noticeable Symptoms?
Yes, dry eye can be present without noticeable symptoms. Neurosensory changes, particularly in older adults, may reduce corneal sensitivity enough that patients feel comfortable despite measurable tear film dysfunction. This is why relying solely on patient-reported symptoms misses a significant portion of preoperative disease.
The PHACO study (Trattler et al., 2017), a prospective evaluation of 136 patients undergoing cataract surgery assessment, found that 77% of eyes had corneal staining and 63% had a TBUT of 5 seconds or less, yet many of these patients had not reported dry eye complaints. Routine objective screening before cataract surgery remains essential because asymptomatic dry eye distorts keratometry and topography just as severely as symptomatic disease. Skipping this step risks basing lens calculations on unreliable measurements.
With a confirmed diagnosis in hand, the next step is treating ocular surface disease before finalizing lens calculations.
How Should Dry Eye Be Treated Before Lens Calculations Are Performed?
Dry eye should be treated before lens calculations are performed using a stepwise approach that stabilizes the tear film and restores consistent corneal measurements. Key strategies include lubricants, anti-inflammatory drops, and in-office gland therapies.
How May Artificial Tears and Anti-Inflammatory Drops Help?
Artificial tears and anti-inflammatory drops may help by restoring tear film consistency and reducing the ocular surface inflammation that distorts preoperative measurements. Preservative-free artificial tears replenish the aqueous and lipid layers, smoothing corneal irregularities that compromise keratometry readings. When inflammation is a contributing factor, your ophthalmologist may recommend prescription anti-inflammatory drops to address the underlying disease process more directly.
According to a 2021 study published in BMC Ophthalmology (Kim et al.), short-term treatment with topical 0.05% cyclosporine A and 0.5% loteprednol etabonate for two weeks prior to cataract surgery yielded significantly improved postoperative refractive outcomes over untreated patients. This combination targets both lubrication deficits and inflammatory mediators simultaneously. For most preoperative patients, starting with preservative-free tears and escalating to prescription anti-inflammatories when needed represents the most practical first-line protocol.
When Should Meibomian Gland Expression or Thermal Treatment Be Used?
Meibomian gland expression or thermal treatment should be used when evaporative dry eye from meibomian gland dysfunction is the primary driver of tear film instability, and when other methods like warm compresses or intense pulsed light (IPL) have not worked. Blocked or atrophied meibomian glands fail to deliver adequate lipid to the tear film, and no amount of artificial tears can compensate for a structurally deficient oil layer.
In-office procedures, such as manual gland probing, thermal pulsation therapy, or intense pulsed light treatment, work by clearing obstructed glands and restoring healthy meibum secretion. According to Donaldson et al. (2022) in the Journal of Cataract and Refractive Surgery, optimizing the ocular surface by diagnosing and treating dry eye disease prior to cataract surgery is important before premium or toric IOL calculations, where even minor tear film irregularity can compromise surgical planning. Patients with visually significant ocular surface disease should be reevaluated for repeat biometry two to six weeks after initiating dry eye treatment to confirm ocular surface stabilization.
How Long Should Dry Eye Be Managed Before Repeating Measurements?
Dry eye should be managed for a minimum of two to six weeks before repeating biometric measurements. This timeline allows the ocular surface to stabilize after treatment initiation, ensuring that keratometry and topography readings reflect the true corneal shape rather than transient tear film disruption.
The exact duration can vary depending on disease severity. Mild cases treated with preservative-free lubricants alone may stabilize sooner, while moderate to severe disease requiring anti-inflammatory therapy or meibomian gland procedures often needs the full treatment window. Repeat measurements should demonstrate consistent, reproducible values across sessions before your surgeon finalizes the IOL selection. Rushing this step remains one of the most common yet preventable sources of refractive surprise in cataract surgery.
With the ocular surface optimized, understanding how cataract surgery itself may worsen dry eye helps set realistic recovery expectations.
How Does Cataract Surgery Itself Worsen Dry Eye During Recovery?
Cataract surgery itself worsens dry eye during recovery through corneal nerve disruption, microscope light exposure, and possible preservative-containing postoperative drops.
How Do Corneal Incisions Affect Tear Film Stability Postoperatively?
Corneal incisions affect tear film stability postoperatively by severing corneal nerves that regulate tear production. According to a 2025 review in Frontiers in Medicine (Nuzzi et al.), corneal nerve disruption during cataract surgery, particularly from clear corneal incisions, leads to a significant reduction in corneal sensitivity and a subsequent decrease in the basal tear secretion rate.
When those nerves lose function, the blink reflex weakens and the signal to produce basal tears diminishes. Reduced tear breakup time and increased corneal staining have been reported to have been significantly reduced in the early postoperative period, and then generally returned toward baseline by 3 months, with some variability. Evaporative dry eye compounds this problem further, as it is more frequently associated with irregular astigmatism on corneal topography, directly compromising toric IOL alignment accuracy. Surgeons who anticipate this nerve recovery timeline can plan lubrication protocols that protect both comfort and visual outcomes.
How Does Microscope Light Exposure Contribute to Inflammation?
Microscope light exposure contributes to inflammation, potentially via oxidative mechanisms, on the ocular surface during cataract surgery. According to an American Academy of Ophthalmology editor’s choice review, the intense light of the operating microscope can damage delicate surface cells, contributing to postoperative tear film instability and goblet cell loss.
Goblet cells produce mucin, the innermost layer that anchors the tear film to the corneal epithelium. When these cells are depleted, tears spread unevenly and evaporate faster. Although surgeons minimize exposure time and use filters, some degree of phototoxic stress is difficult to eliminate entirely. This inflammation typically overlaps with the nerve disruption caused by incisions, creating a compounding effect in early recovery.
How Do Preservatives in Postoperative Eye Drops Aggravate Dryness?
Preservatives in postoperative eye drops aggravate dryness by damaging the corneal epithelium during a period when the ocular surface is already compromised. Benzalkonium chloride (BAK), the most common preservative in ophthalmic drops, has been associated with clinical signs of ocular surface disease, corneal epithelial changes, tear film instability, and staining.
Patients typically use multiple preserved drops simultaneously after surgery, including antibiotics, anti-inflammatories, and corticosteroids. This cumulative preservative exposure can impact the already fragile tear film. Preservative-free formulations offer a practical alternative that may reduce this additional burden on the healing ocular surface.
With these surgical factors in mind, understanding the broader risks of ignoring dry eye before surgery becomes essential.
What Are the Possible Risks of Ignoring Dry Eye Before Surgery?
The possible risks of ignoring dry eye before surgery include refractive surprise and compromised premium IOL performance. The sections below cover how untreated dry eye can lead to unexpected postoperative vision errors and why multifocal lenses are especially vulnerable.
How Could Untreated Dry Eye Lead to a Refractive Surprise?
Untreated dry eye could lead to a refractive surprise by introducing measurement errors during preoperative biometry that carry forward into IOL power selection. When the tear film is unstable at the time of keratometry and topography, the corneal curvature readings captured may not reflect the eye’s true optical power. The surgeon then selects a lens based on flawed data, and the patient wakes up with an unintended prescription.
Refractive surprise after cataract surgery is significantly more common in patients with untreated dry eye, with some reports indicating a postoperative spherical equivalent error exceeding 0.5 D from the intended target. Even half a diopter of unexpected error can mean the difference between spectacle independence and persistent blur. This is one of the most preventable complications in modern cataract surgery, yet it remains common precisely because dry eye is underdiagnosed at the preoperative visit.
How Might Ignoring Dry Eye Affect Premium or Multifocal IOL Outcomes?
Ignoring dry eye may affect premium or multifocal IOL outcomes by degrading the optical precision these advanced lenses require to function correctly. Multifocal, extended depth of focus, and toric IOLs split or redirect light through engineered zones on the lens surface. Even minor tear film irregularities scatter incoming light before it reaches these zones, reducing contrast sensitivity and introducing visual disturbances such as halos and glare.
Preexisting dry eye disease is associated with a significantly higher rate of higher-order aberrations postoperatively, which directly compromises image quality from multifocal and EDOF IOLs. When dissatisfaction mounts, lens exchange sometimes becomes necessary. In a study of 29 patients (35 eyes) that underwent multifocal IOL exchange, Kim et al. (2017) reported that the most common reason for exchange was blurred vision at 60%, frequently linked to uncorrected ocular surface disease. For patients investing in premium lenses, untreated dry eye can effectively negate the visual benefits they expected to gain.
Understanding these risks reinforces why ocular surface optimization should precede any lens power decision.
Who Is Most at Risk for Dry Eye Complications Around Cataract Surgery?
The patients most at risk for dry eye complications around cataract surgery include older adults, those with autoimmune conditions, and long-term contact lens wearers. Each group faces distinct challenges that can compromise preoperative measurements and postoperative healing.
How Does Age Increase Dry Eye Risk Before and After Surgery?
Age increases dry eye risk before and after surgery because tear production and meibomian gland function decline progressively with time. According to a 2017 study in Clinical Geriatrics Medicine (Baer & Walitt), dry eye symptoms are reported by up to 30% of persons over the age of 65, with a significantly higher prevalence observed in women compared to men.
This age-related decline means that many older cataract candidates already have a compromised ocular surface before they ever reach the surgical suite. Since unstable tear films distort keratometry and biometry readings, older patients often benefit from preoperative dry eye treatment before final lens calculations are performed. In clinical practice, treating the ocular surface first is one of the most overlooked steps for improving refractive outcomes in this population.
How Do Autoimmune Conditions Affect Surgical Dry Eye Risk?
Certain autoimmune conditions affect surgical dry eye risk by causing chronic inflammation that reduces tear production and damages the ocular surface. Conditions such as Sjögren’s syndrome, rheumatoid arthritis, and lupus can significantly worsen both preoperative measurement accuracy and postoperative recovery.
Sjögren’s syndrome is particularly relevant. Approximately 10% of patients presenting with clinically significant dry eye disease are found to have underlying Sjögren’s syndrome, a systemic autoimmune condition requiring multidisciplinary management, according to a 2023 report from the American Academy of Ophthalmology. Because autoimmune dry eye tends to be persistent and severe, these patients may need longer treatment courses before biometry readings stabilize enough for reliable lens power selection. For patients with known autoimmune disease, coordinating care between the ophthalmologist and specialized doctor often produces better surgical outcomes.
How Does Long-Term Contact Lens Wear Raise Dry Eye Risk?
Long-term contact lens wear raises dry eye risk by altering meibomian gland structure and destabilizing the tear film over time. Long-term contact lens wearers exhibit a significantly higher prevalence of meibomian gland dropout and tear film instability, with up to 50% of lens wearers reporting dry eye symptoms that can complicate preoperative cataract measurements.
Years of lens wear can reshape the corneal surface in subtle ways that compound the measurement challenges the dry eye already creates. This combination makes accurate keratometry and topography readings especially difficult to obtain without first stabilizing the ocular surface. For longtime lens wearers approaching cataract surgery, discontinuing lenses well in advance and completing a targeted dry eye treatment protocol may help ensure more reliable biometric data.
With these risk factors identified, managing dry eye during the recovery period becomes the next essential step.
What Can Patients Do to Manage Dry Eye During Cataract Surgery Recovery?
Patients can manage dry eye during cataract surgery recovery by following a structured postoperative treatment plan and understanding realistic healing timelines. The subsections below cover which treatments may speed healing and how long post-surgical dryness typically lasts.
Which Postoperative Dry Eye Treatments May Speed Healing?
Postoperative dry eye treatments that may speed healing include preservative-free artificial tears, anti-inflammatory drops, and consistent follow-up care with your ophthalmologist. According to a 2008 report in Ophthalmology Management, aggressive perioperative management of the ocular surface, including preservative-free lubricants and anti-inflammatory agents, has been shown to resolve surgical-induced dry eye in the majority of patients by 6 months postoperatively.
Key treatments your eye doctor may recommend include:
- Preservative-free artificial tears applied frequently throughout the day to maintain tear film stability.
- Anti-inflammatory eye drops, such as cyclosporine or lifitegrast, to reduce ocular surface inflammation.
- Warm compresses and lid hygiene to support meibomian gland function and lipid layer quality.
- Avoiding preserved eye drops when possible, since preservatives like benzalkonium chloride can worsen epithelial damage during early recovery.
Starting treatment early, rather than waiting for symptoms to become severe, gives the ocular surface the best chance of stabilizing before discomfort interferes with daily life.

How Long Does Post-Surgical Dry Eye Typically Last?
Post-surgical dry eye typically lasts one to three months for most patients, though symptoms can persist for 6 to 12 months in some cases. According to a 2025 report in The Ophthalmologist, postoperative dry eye symptoms typically peak within the first week after cataract surgery, with 8% to 48% of patients continuing to experience issues up to the six-month mark post-surgery.
Several factors influence recovery duration:
- Pre-existing dry eye severity before surgery, which affects the baseline the ocular surface must recover from.
- Corneal nerve healing time, since sensory disruption from the incision temporarily reduces natural tear production.
- Adherence to the postoperative treatment plan, including consistent use of lubricants and anti-inflammatory agents.
Patients with underlying conditions such as Sjögren’s syndrome, which affects approximately 10% of those with clinically significant dry eye, may require longer and more specialized management. Most patients who follow an active recovery protocol, however, can expect meaningful improvement within the first few months.
With a clear recovery strategy in place, understanding how dry eye fits into the broader surgical journey helps patients prepare with confidence.
How Can Patient Education Help You Prepare for Cataract Surgery With Dry Eye?
Patient education can help you prepare for cataract surgery with dry eye by clarifying how ocular surface health directly influences lens selection accuracy and visual outcomes. The sections below cover how Eye Surgery Today’s guides support informed decisions and the key takeaways from this article. Beyond cataract-specific considerations, patients may also benefit from understanding other available vision correction procedures, such as LASIK refractive surgery, to make fully informed decisions about their eye health.
Can Eye Surgery Today’s Guides Help You Understand Dry Eye and Lens Selection?
Yes, Eye Surgery Today’s guides can help you understand dry eye and lens selection by translating complex surgical concepts into clear, actionable information. Dry eye affects the measurements your surgeon relies on to choose the right intraocular lens, yet many patients are unaware of this connection before their procedure. A Cullen Eye Institute study at the Baylor College of Medicine examined 29 patients (35 eyes) that underwent multifocal IOL exchange, reporting that the most common reason for exchange was blurred vision at 60%, frequently linked to uncorrected ocular surface disease (Kim et al., 2017). Understanding this relationship before surgery is one of the most effective steps a patient can take to protect their visual investment. Eye Surgery Today provides educational resources, including guides on IOL options and preoperative preparation, designed to help patients recognize when dry eye needs treatment before lens calculations are finalized.
What Are the Key Takeaways About How Dry Eye Affects Lens Calculations and Recovery?
The key takeaways about how dry eye affects lens calculations and recovery are:
- An unstable tear film distorts keratometry and topography readings, which can lead to incorrect IOL power selection.
- Untreated dry eye increases the risk of refractive surprise and can increase postoperative spherical equivalent error, sometimes exceeding 0.5 D from the intended target.
- Cataract surgery itself can worsen dry eye through corneal nerve disruption, microscope light exposure, and preservative-containing postoperative drops.
- Preoperative dry eye treatment followed by repeat biometry improves measurement accuracy and visual outcomes.
- Premium and multifocal IOLs are especially sensitive to ocular surface irregularities, making dry eye management essential before selecting these lenses.
For most patients, the single most impactful action is ensuring dry eye is diagnosed and treated before biometry measurements are taken. Eye Surgery Today’s educational resources can guide you through each stage of this process, from understanding your diagnosis to preparing for a confident conversation with your surgeon.
